


COVID Transmissions for 10-15-2020
Original Antigenic Sin and COVID-19

Good morning! It has been 333 days since the first documented human case of COVID-19. We’re very close to the 3-month mark for this newsletter. It will pass over the weekend, this Saturday, so raise a toast to COVID Transmissions if you get a chance.
Today I’d like to expand upon the concept of Original Antigenic Sin in an in-depth piece.
As usual, bolded terms are linked to the running newsletter glossary.
Keep the newsletter growing by sharing it! I love talking about science and explaining important concepts in human health, but I rely on all of you to grow the audience for this:
Now, let’s talk COVID.

Another case of symptomatic reinfection; this time, with a death
It has been reported widely that a Dutch woman recently had a reinfection with SARS-CoV-2 that led to disease and death.
Again, I don’t think that these cases of reinfection with symptoms are tremendous causes for concern yet. We are still looking at these as relatively uncommon events. That may change as further followup occurs, but speculation is dangerous in many ways.
Barron Trump also tested positive for SARS-CoV-2 infection
First Lady Melania Trump announced today that her son, Barron Trump, also tested positive for SARS-CoV-2 infection, but did not display symptoms.
This makes the Trump cluster an interesting case study in how this disease affects different people. In this cluster, you have a large number of middle-aged individuals who became infected, including the First Lady. You also have one older individual who was infected, and at least two young people—Barron Trump and Kellyanne Conway’s daughter Claudia.
The results of these infections were rather in line with what we might expect from the wider national experience. President Trump experienced a somewhat serious case of COVID-19, requiring hospitalization. Since he is the President, a number of high-intensity interventions were taken, which appear to have helped keep the clinical course of his disease on track.
In the middle-aged individuals infected, including the First Lady, there were some reports of symptoms and some reports of asymptomatic disease. The First Lady, being young and a woman, seems to have had the experience we would expect for being in two relatively low-risk groups. She experienced mild symptoms, but there was some disease present. She reportedly has recovered. This is in line with expectations. I suspect that she would have received much the same care and urgent attention that the President himself received, had her disease been more severe.
And then you have the younger individuals, who have experienced either mild or no disease. Details on Claudia Conway’s condition are sparse, but Barron Trump is reported not to have experienced any symptoms at all.
The political drama aside, this is an infectious cluster that we can use to understand how COVID-19 may proceed in people who have access to the very best of medical care. The most severe disease in the elderly might still be treatable, while in younger individuals cases of severe disease would be more rare.
If there’s anything we can learn from this, it’s that if you’re in President Trump’s age group, and you get sick during this pandemic, don’t wait to talk to a doctor.

What am I doing to cope with the pandemic? This:
Braised collard greens
Collard greens are hard to make on a kosher diet. They normally call for a large volume of something rather nonkosher. On the other hand, I happen to like the greens themselves and recently got some from our farm share delivery. What’s a virologist to do?
Something that I’ve been using a lot of during the pandemic is liquid smoke. It’s a great ingredient if you want barbecued flavor without having the ability to barbecue. As it turns out, bacon is kind of smoky. But it’s not exclusively smoky; there’s also a sweetness to pig-based products as well as a more savory element that’s hard to pin down.
To create my simulated authentic collards, I roughly chopped some onions and garlic, which were then sautéed together for a few minutes. The collard greens themselves were also given this same treatment after the onions had turned translucent and started to caramelize a little.
Something that’s important for tough greens is to get them tender. A great way to make vegetables tender is braising, but particularly you can get a nice effect with collard greens if you add a little acid to the pan. So, I used apple cider vinegar, which I thought would add the sweet-sour element, and also helped to deglaze the pan a little bit. To this I added some salt, and enough of the liquid smoke to get the flavor of it through without overpowering everything else. That amount is dependent upon the brand you’re using so I’m not going to pretend to estimate.
I let this braise, covered, for about 20-30 minutes until the greens had lost their brightness. I’m afraid this is a little unavoidable; with collard greens keeping them bright usually means they’re going to also stay tough, which you definitely don’t want.
I thought this preparation worked well and gave the right kind of smoky-sweet flavor I was looking for.

Original Antigenic Sin and COVID-19
Today I’d like to walk through a new paper—a preprint—that I recently saw. Most of you will know that I don’t like to cover preprints in this newsletter because they haven’t been peer-reviewed, but I found this one particularly interesting.
In the past, we’ve discussed the concept of “Original Antigenic Sin.” This is an old idea in viral immunology, observed in viruses like influenza virus where a wide variety of strains exist that produce immunity that is not quite good enough for a response to one strain to be protective against another. What we see in these viruses is that the immune response is strongly biased towards the first virus from that species that a person is infected with during their lifetime. Antibodies are produced that strongly respond even to subsequent, less-related strains. Often, these antibodies do not provide adequate protection—and they may not provide any protection at all.
Original antigenic sin has equivalents in other pattern-recognition systems. For example, humans as pattern recognition systems have all kinds of horrible biases related to our first experience of something. How many people still hate Brussels sprouts, for example, due to a bad experience with them as a child? As it turns out, Brussels sprouts as many of us have known them as children no longer exist. The cultivar that was common before the late 1990s was extremely bitter and much-hated by children. A first experience with that variety has turned off a lot of people to the whole species, because many who had it developed a heuristic reaction that Brussels sprouts are to be avoided. As it turns out, since then, agricultural botanists have developed a much less bitter cultivar, which is now sold around the world. It’s delicious, and has helped the vegetable’s popularity to increase. If you’re still one of the holdouts who believes that Brussels sprouts are inedible, you may want to try them now. You may be a victim of something like Original Antigenic Sin, in its psychological equivalent. All pattern recognition systems are vulnerable to this type of heuristic-based bias. The immune system is no exception.
For SARS-CoV-2, it wouldn’t be expected that Original Antigenic Sin would play a big role. This is a virus that doesn’t naturally circulate in humans, at least not until 2020, and so it wouldn’t be anticipated that a previous strain would exist to create such a bias.
However, as I’ve communicated in the past, researchers have found that seasonal human coronaviruses, which are a few of many causes for the common cold, can generate immune responses that have a certain cross-reactivity with SARS-CoV-2. Specifically, it has been shown that T-cells that react to human coronaviruses can cross-react to recognize SARS-CoV-2.
At the time that I shared this discovery with this newsletter, I cautioned that this doesn’t tell us anything about the clinical course of disease in patients who have such T-cells. On the one hand, it’s possible that these T-cells help the immune system to better fight SARS-CoV-2. On the other hand, it’s possible that their existence prevents the development of specific T-cells that might better fight SARS-CoV-2.
When I first heard about this finding, I wondered if perhaps the age-related severity of COVID-19 could be a product of these off-target memory responses. What if the only reason that older people are more likely to have severe disease is that they have more historical responses to human-adapted seasonal coronaviruses, which bias their immune system away from mounting a proper response to SARS-CoV-2? What if the reason that children are less likely to be symptomatic is that they have not seen enough human-adapted coronaviruses to have these biasing responses?
Until now, these questions have been without answer. This new preprint offers us some insights on potential answers, however.
In this work, the researchers explored preexisting antibody responses to seasonal human coronaviruses. They looked at 17 patients with severe COVID-19 and dissected the various components of their immune response, characterizing a wide panel of antibodies that reacted to various SARS-like coronaviruses. These patients had antibodies that appeared rapidly and that cross-reacted with SARS-CoV-2, MERS (another bat-borne coronavirus that can cause disease in humans), and also with human coronaviruses. The authors determined that while new and specific antibodies were generated in these patients that reacted to components of SARS-CoV-2, there was also a large population of other antibodies, from apparent immune memory responses, that were also generated during the infection. The authors demonstrated that these antibodies reacted most strongly with seasonal human coronaviruses.
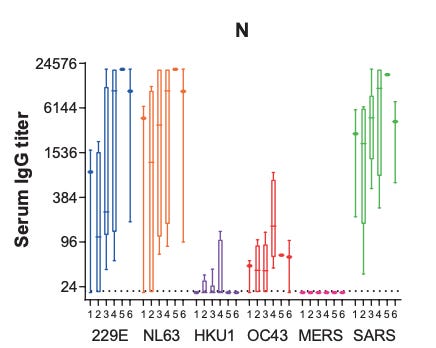
Image is a representative figure from the paper. The rightmost category shows antibodies responding to SARS-CoV-2, while the other groups show reactivity to other coronaviruses over time during infection with SARS-CoV-2. In this example, it is evident that antibodies reacting to other coronavirus species increase in signal during infection with SARS-CoV-2.Importantly, these antibodies did very little to neutralize SARS-CoV-2, despite their cross-reactivity. They seemed to be a strong, useless response based on past exposure to a similar virus species. This appears to be evidence of original antigenic sin, apparently documented as a phenomenon in patients with severe COVID-19.
I have to caveat this substantially. We are talking about 17 patients here, and we don’t have any kind of control group. For all we know, you see the same pattern in patients who do not have any kind of severe disease. For all we know, this has nothing at all to do with severe disease and the SARS-CoV-2-specific antibodies that are detected in these patients would have been sufficient to provide protection if it were not for some other, unknown disease effect that occurs in patients with severe cases. I don’t want to overly speculate; please realize that the scientific process is full of false starts and misleading hints, and this may just be another one of those.
On the other hand, this leans toward the possibility that past exposure to coronaviruses that circulate in humans might somehow impact severity of COVID-19 through a mechanism similar to Original Antigenic Sin, and for that reason I think it’s a finding to watch. I am eager to see where followup on this enticing hypothesis may lead.
If you’d like, you can read the full paper, but keep in mind it has not been peer-reviewed: https://www.medrxiv.org/content/10.1101/2020.10.10.20210070v1.full.pdf

Join the conversation, and what you say will impact what I talk about in the next issue.
Also, let me know any other thoughts you might have about the newsletter. I’d like to make sure you’re getting what you want out of this.

This newsletter will contain mistakes. When you find them, tell me about them so that I can fix them. I would rather this newsletter be correct than protect my ego.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.
Thanks for reading, everyone!
See you all next time.
Always,
JS