


COVID Transmissions for 11-23-2020
Do we get immune memory in COVID-19?

Good morning! It has been 372 days since the first documented human case of COVID-19. Welcome back from another weekend.
In today’s in-depth, I walk through the next figure of a paper we have been looking at, which tried to understand how long immunity against SARS-CoV-2 may last. In the first in-depth on this topic, we saw that antibodies against the virus can last for a good period of time. Today, we’re going to ask about the immune cells that remember past infections and create antibodies to fight them.
Also, some headlines.
In part because I attended a virtual convention this weekend, I know there are a lot of new readers here today. I hope you enjoy this newsletter, and I hope it helps you navigate the pandemic a bit better. If it does, I encourage you to share it with friends, family, and anyone else you think might enjoy it.
As usual, bolded terms are linked to the running newsletter glossary.
Keep the newsletter growing by sharing it! I love talking about science and explaining important concepts in human health, but I rely on all of you to grow the audience for this:
Now, let’s talk COVID.

Worldwide, spread of COVID-19 is still bad
We have exceeded 58.5 million documented infections worldwide, with 1.39 million deaths identified.
In the US, we are at 12.3 million cases with around 257,000 deaths. With little national-level attention and the impending Thanksgiving holiday, I expect things are not going to trend any better in the US anytime soon.
In Europe, the recent surge appears to be starting to stabilize, but that does not mean that Europeans are out of the woods.
FDA Emergency Use Authorization for a rapid at-home COVID-19 test
Last week, the FDA approved a rapid, at-home test for infection with SARS-CoV-2: https://www.popsci.com/story/health/coronavirus-home-test-fda/
This is not exactly the type of test that I’m still hoping for, but it is another tool in our arsenal. This test will still detect RNA from the virus, instead of detecting virus itself. However, it uses a technology that is fast and easy, and doesn’t require complex lab equipment, making it possible to use at home.
This test will require a prescription, which also isn’t ideal. Still, this could be useful for the monitoring of patients who are in quarantine due to potential exposure or appearance of symptoms. It is better than needing to bring potentially infected patients into a clinic for repeated testing, and may offer some relief to overburdened testing facilities. All in all, a small piece of good news.
Pfizer applies for Emergency Use Authorization for its vaccine
On Friday, Pfizer applied to the FDA for Emergency Use Authorization for its COVID-19 vaccine. The FDA has until December 10th to provide its decision on this. I expect that the vaccine will be authorized for use in healthcare workers at first, and potentially also high-risk patients. We will know soon.
The first doses will likely be delivered in December.
CNN has more details here: https://www.cnn.com/2020/11/20/health/pfizer-vaccine-eua-submission/index.html

What am I doing to cope with the pandemic? This:
Philcon
Philcon, better known as the Philadelphia Science Fiction Convention, was this past weekend. I’ve been a guest at Philcon for five years now, largely doing science programming. Science conversations are a pillar of the science fiction convention circuit, for both professional and entertainment reasons. Ironically, my first Philcon panel ever was entitled “Epidemic,” and you can imagine that this year that theme came up a lot too.
This year, in fact, I felt was the most important Philcon I’ve ever attended. While the convention had to be virtual due to the ongoing pandemic, there were a number of program items in which I participated that offered opportunities to educate about COVID-19. One allowed me to demonstrate the proper use of an N95 mask. This is information that is not only interesting but might have a direct, lifesaving impact.
You might have guessed that I strongly believe in and enjoy science education, and it was great to be able to be a part of it this weekend once again.

Estimating the duration of immunity against SARS-CoV-2 — Part 2, B cells
I’m picking back up where I left off in Friday’s newsletter, walking through a recent paper about the duration of immunity in SARS-CoV-2. Last time (11-20-2020, for those just joining us now), I discussed the design of the study and we walked through the first figure in the paper, which established that antibodies are generated against SARS-CoV-2 in the large majority of infected patients, and that these antibodies are likely maintained for a long period of time.
For those following along, again, the paper can be found here: https://www.biorxiv.org/content/10.1101/2020.11.15.383323v1.full.pdf
That alone would have been a worthy topic for a paper. However, these authors went a step further. A couple of steps, in fact.
Antibodies are a weapon in the immune system. They are produced in large quantities to fight off active infections, but they don’t come out of nowhere. They’re made by cells. Specifically, the cells that produce antibodies are known as B cells, a type of white blood cell.
B cells don’t just produce antibodies. They also improve the quality of antibodies by literally mutating them during the course of infection, and what’s more, they develop memory populations that help us respond better to the infection the next time it comes the body’s way. These memory cells are stored in the body and when an infectious agent appears again in the future, they divide quickly and expand their population to produce large quantities of antibodies and mount a strong defense.
Antibodies decline after infection, but memory B cells are there to make more of them again if we are challenged by the same pathogen again.
The first questions that were asked in this paper were about antibody production. Having answered those, the authors moved on to the next logical question: what about B cells?
Specifically, the authors wanted to ask the following list of questions about B cell populations:
Are memory B cells generated following SARS-CoV-2 infection?
If yes, what types of memory B cells are generated?
B cells tend to specialize in the types of antibodies that they make; what types of antibodies do the memory B cell populations create?
What parts of the virus do these memory populations target?
How long do these B cell populations last?
These are really sophisticated scientific questions, so we’re going to have to strap in to revisit some concepts before we answer these questions. One thing I want to introduce you to is an experimental technique called flow cytometry. Flow cytometry is an amazing tool, particularly for immunologists. “Cytometry” just means “measurement of cells.” The “flow” part comes from how the technique works; a mixed population of cells, suspended in fluid, is pushed past a series of electronic “gates” that filter cells out based on their surface characteristics—cells are sorted and measured as they “flow” past. Surface characteristics are a big deal for immune cells; it’s how we identify them. And B cells are no exception.
Through the use of careful “gating strategies,” we can sort cells according to the type of cell they are, they type of antibodies they produce, and even what those antibodies target. This allows us to study immune cells very closely, and create figures like this panel:

I recognize this looks weird; I’ll walk you through it.
In this figure, we are looking at flow data where memory B cells were sorted out of the wider population of cells. Each dot represents a cell. Each of these pictures is a sample that has been analyzed from an individual patient, showing their memory B-cell population. What happens here is that the cells have been sorted according to increasing affinity for specific antigens, so that as you move upward and to the right in the graph, you see cells that have increasing ability to recognize the specific antigens being studied.
Simply put, the more you go up and to the right on these graphs, you see cells that more strongly recognize parts of the SARS-CoV-2 virus. We are seeing the B-cell populations sorted by how strongly they recognize the virus.
The “unexposed” set of images is a typical patient who has not been infected with SARS-CoV-2; as you can see, this patient does not have a lot of cells that have affinity for what is being examined. Specifically, the researchers looked for affinity to the spike glycoprotein of SARS-CoV-2, a key immune target that is also at the center of vaccine design, as well as the nucleocapsid protein, a protein that coats the SARS-CoV-2 genome. In the unexposed patients, there is no substantial cell population that recognizes either of these. Some cells do come up; this is partly because B cells have a wide range of things that they recognize, so they can develop in response to any infection, and also partly because experimental setups can be imprecise. However, we see the enclosed red areas that count the density of cells detected. The numbers there are very low.
The researchers went a little deeper in looking at the spike protein; not only did they look at general recognition of the spike protein, they also looked at cells that recognize a subpart of the spike protein—specifically, the receptor-binding domain (RBD). We have talked about the RBD before; it is a key target for immunity because it controls attachment of the virus to cells. Here, they took the population of cells that recognized the spike and further sorted them for recognition of the RBD. Again, in the “unexposed” patients, there is nothing substantial that recognizes the RBD.
In the COVID-19 condition, we see data from 3 typical patients who were infected with SARS-CoV-2. In these, we see a big projection of cells that recognize spike, spike RBD, and nucleocapsid. Those are the dots that project up and to the right. We also see the quantification of these cells, enclosed inside the red boxes. The numbers here are much higher than for the unexposed patient.
These are representative images. The researchers did these experiments in almost 200 patients, to catalog their responses to SARS-CoV-2, and understand how memory B cell populations appear. We will look at the data in the aggregate in a moment, where it may be a little more approachable. However, we have begun, in this figure, to answer our first question: Are memory B cells generated following SARS-CoV-2 infection? Signs point to yes.
This also gives us our first look at part of our second question, regarding which parts of the virus the memory B cells recognize. We’re doing well with our experiments so far!
However, we also wanted to know about the types of antibodies being recognized. I’d like to walk through what I meant by that.
Last time, we talked about different types of antibodies. We discussed the common, blood-resident antibodies known as IgG, which are really a workhorse of the immune system. We also discussed the more specialized IgA antibodies, which are known as “mucosal” antibodies and respond to infections at mucosal surfaces—tissues like the respiratory tract that interface between the inside of our bodies and the exterior environment. One type that we did not discuss was the IgM antibody.
IgM antibodies are the first type produced during an active infection. They are an unusual type of antibody, and more primitive than the specialized IgG and IgA. IgM antibodies evolved first, and at some point in the history of our evolution, we developed the other types of antibodies, but not as separate products. Instead, to make IgG and IgA, B cells mutate their own genomes, on the fly, to do something called “class switching.” They change themselves from producing IgM to producing IgG, IgA, or other types of antibodies that are not within the purview of this piece right now. It’s an incredible mechanism.
B cells also mutate themselves in other ways, through a process called “affinity maturation.” The parts of the B cell genome that code for the antigen-specific part of the antibody actually mutate, at about a million times the mutation rate of cells in the rest of the body, to improve the way that antibodies are targeted.
Interestingly, memory B cell populations set aside B cells from various steps along this process. IgM-producing cells become memory cells, as do IgG- and IgA-producing cells. Setting aside the more “primitive” IgM memory cells may allow a certain amount of flexibility in future immune responses, creating room for the maturation of a new response if a similar pathogen is seen in the future, but with some differences relative to the first infection. There are a lot of advantages to this; sometimes, pathogens mutated. Other times, a pathogen could infect by one route the first time around but another route in the second infection—for example, the smallpox vaccine involves creating an infection in the skin (actually with a different, related virus), but the actual infections that it protects against are caused by inhalation of virus. By keeping a diverse population of memory B cells, the immune system maintains agility to respond to somewhat unexpected situations.
The reason I’ve gone down this road of explanation is to show you the following figure:
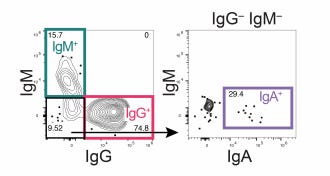
Here, again, we are looking at flow cytometry. The researchers separated spike-recognizing memory B cells according to the type of antibody they made. We see all the major types here! There is a defined population of IgM-expressing spike-specific B cells. There is a very large population of IgG-expressing spike-specific B cells. In the remaining population of cells, we see a nice amount of IgA-expressing spike-specific B cells; it’s smaller than the IgG or IgM populations, but it’s there!
In straightforward terms, we have a diverse population of B cells, representing the capabilities to produce various antibody types that respond to virus infections. That’s good news.
I’ve shown you some things that I imagine weren’t easy to understand at first—this is sophisticated, cutting-edge science—but we’ve approached answers to the questions we wanted to ask at the outset. We know that memory B cells are generated in response to SARS-CoV-2 infection. We learned that they recognize diverse parts of the virus, both the spike protein as well as the nucleocapsid, which respectively are expressed on the outside and the inside of the virus particle. We learned that these memory B cell populations contain cells that express IgM, IgA, and IgG antibodies—a diverse repertoire of antibody products that can respond to infection in different ways.
We have one question left, and for that we have to look at the results of the flow cytometry in the aggregate. Let’s look at this figure:

The quick interpretation of the data here is that we seen memory B cells, recognizing the spike protein, developing within 30 days of symptom onset. We then see these populations grow slightly over the next month or so until they reach a stable level. They do not appear to shrink over time, at least not substantially. There is what appears to be a lasting memory response, at least on this time scale.
The work here was conducted in the “cross-sectional” experiment population, patients from whom only one sample was obtained. This is as opposed to the “longitudinal” sample, where patients had two samples collected at different times. The former gives us a sense of how the immune response develops in large numbers of people, but it doesn’t show us necessarily how it changes in individuals over time; we get some information on that from the longitudinal sample, but the number of people in that sample is smaller.
The researchers also looked at the longitudinal sample. In these patients, also, the populations of memory B cells increased over time, with only slow decay apparent. This is good news.
The researchers took this further, looking at cells that recognized the spike RBD and also cells that recognized the nucleocapsid. They then looked at subpopulations of this list, looking at spike-, RBD-, and nucleocapsid-specific memory cells that expressed IgM, IgG, and IgA. Long story short, in each of these populations, they saw a quick rise in memory B cells.
However, the specific subtypes—IgA, IgG, and IgM—saw a little decrease in cell populations over time. It appeared that IgM-expressing B cell populations decreased the most quickly; this makes sense, since as infection resolves these tend to go away. IgA-expressing B-cells also went down over time, but the data are noisier because there are fewer of these cells. IgG-expressing B cells only decayed a little bit over time.
We would expect some decline in these specific populations. They don’t seem to disappear, either, though. This is fine—B cells, like all cells, can divide to make more copies of themselves. When a new SARS-CoV-2 infection appears, I expect them do just that, and mount a strong and full response to this second infection, providing protection against disease.
Let’s return to our questions from the beginning:
Are memory B cells generated following SARS-CoV-2 infection?
If yes, what types of memory B cells are generated?
B cells tend to specialize in the types of antibodies that they make; what types of antibodies do the memory B cell populations create?
What parts of the virus do these memory populations target?
How long do these B cell populations last?
Yes, memory B cells are generated following SARS-CoV-2 infection. The memory B cells that are created produce a diverse set of IgM, IgG, and IgA antibodies, all of which would be important in responding to a new infection. These populations recognize diverse parts of the SARS-CoV-2 virus. The memory B cell populations appear to last for quite some time, too, though it’s expected that they will gradually decline over time.
So far, in our walkthrough of this paper, we have seen that antibodies are generated in SARS-CoV-2 infection, and that these antibodies are retained in the body for quite some time. We have also now seen that memory B cells are generated that can replace these antibodies in the event of a second infection. Together these responses likely contribute to protection against COVID-19.
What we have not explored in this paper yet is a third part of the immune system: T cells. The researchers who did this work also asked questions about T cells, and we will cover these experiments in my next in-depth piece.

In response to Friday’s issue, reader Robert Berger left the following comment:
Thank you for the in depth on the Danish study. Some people I know have been citing the claims that this study proves that masks are ineffective. I am using your in depth as a non-confrontational apolitical means of getting people to focus on the actual facts. Very helpful.
Thanks Robert! I think I was a little confrontational, at least…but I’m glad that my analysis has proven useful. It’s always nice to hear.
Now, we went through some advanced scientific work today. You might have some questions! Send them in.
I also want to answer your questions on different topics, so please don’t hold back if you’re interested in asking me anything.
Join the conversation, and what you say will impact what I talk about in the next issue.
Also, let me know any other thoughts you might have about the newsletter. I’d like to make sure you’re getting what you want out of this.

This newsletter will contain mistakes. When you find them, tell me about them so that I can fix them. I would rather this newsletter be correct than protect my ego.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.
See you all next time.
Always,
JS