


COVID Transmissions for 12-13-2021
Vaccine effect against Omicron; vaccine effect against long COVID

Greetings from an undisclosed location in my apartment. Welcome to COVID Transmissions.
It has been 757 days since the first documented human case of COVID-19. The 757, the successor to the 747, is an incredible workhorse aircraft that has been in service for decades and continues to perform exceptionally.
We’re going to be focusing on the Omicron variant for a while, and today’s issue is no exception. However, we also have a story on vaccine-mediated prevention of long COVID, and also a followup on pediatric myocarditis.
Also, a quick heads up that I will be traveling this week and there might not be a Friday issue. I will try, but my schedule is very full. Don’t be alarmed if I miss Friday.
Bolded terms are linked to the running newsletter glossary.
Keep COVID Transmissions growing by sharing it! Share the newsletter, not the virus. I rely on you to help spread good information, which you can do with this button:
Now, let’s talk COVID.

Omicron variant: early vaccine effectiveness data against disease
Some data on vaccine effectiveness against symptomatic disease caused by the Omicron variant have been floating around the Internet:
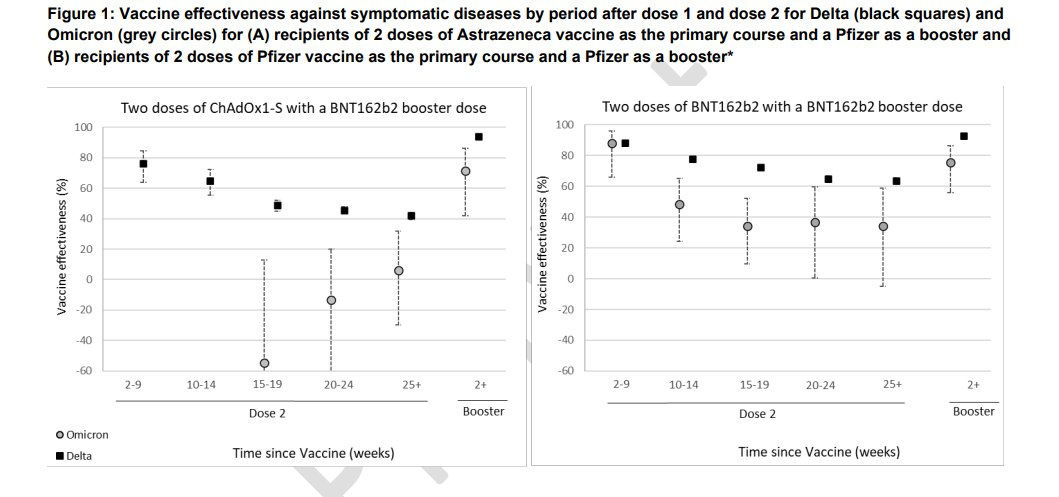
These data come to us from the UK, which has often been a leader in information release when it comes to vaccine efficacy against new variants. However, these are early data and they have small numbers of patients here. I think that is probably the best explanation for the apparent negative vaccine effectiveness of the AstraZeneca vaccine here. I read all of those values as approximately less than 30% effective, and maybe not effective at all—but I do not think these values are representative.
For the Pfizer vaccine we have a different story, but the numbers here are still small. The vaccine remains substantially protective against symptomatic disease after 2 doses, but much less than we would like. The booster dose appears to restore protection meaningfully. Based on this, I also expect that effectiveness against severe disease and death will remain high, but it’s very early days here.
My big takeaway from this is that the human immune system is capable of attacking a virus that has made substantial changes even from the original strain that generated immunity. That’s pretty amazing! However, those substantial changes mean the virus is able to make its presence known again even in the immunized individual.
I’m glad, here, that we are not looking at infection only, but also at symptomatic disease. This is frankly what really matters most. If the virus can make you sick again, that’s what we really need to know here. It appears that, yes, it can make an immunized person sick, with the odds of that happening being determined by the vaccine that they got. There are a lot of vaccines not represented in this particular figure, and again, the error in this is wide because we don’t have a lot of Omicron events/patients to include yet.
The case is, however, mounting for getting a booster dose if they are available in your country. I also believe that this is strongly supportive of mRNA vaccines over other options. I am a little afraid of how inactivated vaccines may perform, like some of the options that have been developed in China. A lot of people around the world have received these, and they had some of the lowest baseline effectiveness of the options out there.
This is a global fight, and it’s clear that we need to make lots of doses of the best vaccines available to as many people as possible, as fast as possible.
By the way, the full report that led to this can be found here: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1040076/Technical_Briefing_31.pdf
Vaccines may be effective at preventing long COVID-19
A truly massive study (240,000+ SARS-CoV-2 infected patients) has looked into the question of whether vaccines can prevent long COVID: https://www.medrxiv.org/content/10.1101/2021.11.17.21263608v1
Because this is a preprint of a retrospective study, before I describe results in summary I want to point out that peer review may substantially change the results. It is rare for peer review to change the results of studies that are designed in advance of the data generation (ie prospective studies), but with retrospective studies, peer reviewers may request different analysis methods because the data already exist. Because the populations are nonrandom, often there is a need for new analyses to control for unbalanced patient characteristics in the different populations being compared. So it’s possible we’ll see a different outcome than what I’m about to describe, but the results are pretty interesting.
One thing I do hope they change on peer review is the use of the phrase “COVID-19 infection.” COVID-19 is a disease, caused by infection with SARS-CoV-2 virus. There is no such thing as “COVID-19 infection.”
In patients who were vaccinated with at least one vaccine dose before SARS-CoV-2 infection, the odds of having two or more long-term symptoms were 7 to 10 times lower than in unvaccinated people. That’s good news!
What’s even more surprising is this—patients who received one vaccine dose within 4 weeks of their SARS-CoV-2 infection also appeared to be somewhat protected from long COVID-19. Such patients were 4-6 times less likely to experience two or more long-term symptoms than the unvaccinated. A 3-fold reduction in risk was also seen in those who got a vaccine dose 4-8 weeks after infection.
If these results bear out over time, it represents an incredible new fact added to the case for vaccination: protection from one of the most fearsome impacts of COVID-19 besides death. I will do my best to follow the story on this one if there are any developments.
Confirmation of no pediatric myocarditis with Pfizer vaccine, after 5 million doses
The CDC has confirmed that in 5 million vaccinations in children, there have been zero reported cases of myocarditis: https://abcnews.go.com/Health/cdc-director-rochelle-walensky-concerns-myocarditis-million-children/story?id=81659883
Looks like they designed that dosage correctly! Glad to see this.

What am I doing to cope with the pandemic? This:
Worldcon
This week, I will be attending Discon III, which also happens to be the 79th World Science Fiction Convention (“Worldcon”). Many of you who read this newsletter are well-versed in the world of science fiction and fantasy conventions, but for those who aren’t, Worldcon is one of the biggest annual events for the SFF world. It is a traveling show, unlike San Diego Comic Con (as an example), and occurs in a different place each year. Since it’s a worldwide convention, the location can be anywhere. It has been in Dublin and Helsinki, both recently.
The far-flung destinations, combined with my having been an exceptionally poor graduate student for quite some time, have meant I never got to go. This year will be my first Worldcon; part of the reason is that this year it is within a 5 hour journey from my home.
Of course, we are entering a particularly dangerous phase of a global pandemic, and you may be wondering why I chose to do this. I think it’s important to share:
I have received three doses of a vaccine against COVID-19 (full vaccination, aka 2 doses with a 2-week waiting period after the second, is required to attend)
I will be using COVID-19 rapid antigen tests every day of the convention, as well as before and after I go
I will be wearing an N95 mask in all public areas, except perhaps the hotel gym (if it’s open and I choose to go), where I may swap it for a surgical mask (masking is required by the convention)
I fully reviewed the convention’s COVID-19 policies and they meet with my approval
None of this is perfect, but taken together it does substantially reduce the risk that I will get COVID-19 or give it to someone else. I do believe that it is appropriate to try to live our lives and take opportunities to do things we’ve always wanted to do—as long as reasonable and expected precautions are put in place.
My 2.5 month old daughter, who is of course not vaccinated, will be staying with her grandparents during the con. One of the reasons we’re able to go to this convention and not others is that she is now old enough to be watched over by close family members for multiple days in a row. She is also the reason I will be testing so frequently. Rapid tests work best when they are used every day, to catch what might have been missed one day on the next. If I test positive, I’ll isolate from her (as well as everyone else), possibly even staying somewhere else until I test negative again.
I’m sure there are those who will disagree with my choice here, but the fact is, we need to find ways to mitigate COVID-19 risk and return life to some sense of normalcy. I believe in modeling that behavior. Masked, vaccinated, and tested is the safest way to live life to its fullest right now; so that’s what I’ll be doing.

While we did have some nice comments on the last issue, we didn’t get to anything that was too informative on COVID-19, so I’ll leave them out this time. Go back and read them if you’re so inclined!
You might have some questions or comments! Join the conversation, and what you say will impact what I talk about in the next issue. You can also email me if you have a comment that you don’t want to share with the whole group.

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.
See you all next time. And don’t forget to share the newsletter if you liked it.
Always,
JS
Enjoy your first WorldCon!
Have fun at WorldCon!