


COVID Transmissions for 12-18-2020

Good morning! It has been 396 days since the first documented human case of COVID-19. We’re going into a weekend—try to enjoy yourselves! But safely, of course.
Today we have several headlines and a response to a reader comment about the closing of restaurants in NYC.
As usual, bolded terms are linked to the running newsletter glossary.
Keep the newsletter growing by sharing it! I love talking about science and explaining important concepts in human health, but I rely on all of you to grow the audience for this:
Now, let’s talk COVID.

Moderna vaccine recommended for approval by FDA advisors
In a vote of 20 yes and 1 abstention, the FDA advisory committee reviewing Moderna’s vaccine recommended that it be authorized.
You can read about this in the New York Times: https://www.nytimes.com/2020/12/17/health/covid-vaccine-fda-moderna.html
Outbreak case study demonstrates that yes, it is possible for COVID-19 to spread in commercial aircraft
In Emerging Infectious Diseases, there is a new study that used genomic analysis to demonstrate definitively that a COVID-19 cluster began with transmission events occurring on a commercial aircraft: https://wwwnc.cdc.gov/eid/article/26/12/20-3910_article
On this flight, 11 patients were SARS-CoV-2 positive at the outset of the flight, 9 of them having become infected during a cruise. These 9 had a genomic lineage of the virus that had not previously been detected in Australia, the flight’s destination, which made it possible to differentiate cases acquired on the flight from potential local acquisition.
At least 8 new cases were associated with the flight. 3 more were identified as possibly associated with the flight.
To me this provides clear evidence that SARS-CoV-2 can be transmitted in commercial aircraft.
Racial bias in pulse oximeter readings
A study in The New England Journal of Medicine highlights that pulse oximeters can give different readings in patients of different races: https://www.nejm.org/doi/full/10.1056/NEJMc2029240
In this study, there was undetected hypoxemia (low blood oxygen) in almost 12% of Black patients, and in only about 4% of white patients. There was a clear discrepancy in the measurement of oxygen saturation by pulse oximetry in Black patients compared to alternative methods of measurement, much more so than in white patients.
The authors of this letter do not make an attempt to describe the potential cause of this issue, but they do reference articles that can explain it, including this approachable one: http://bostonreview.net/science-nature-race/amy-moran-thomas-how-popular-medical-device-encodes-racial-bias
Long story short, pulse oximeters are an optical measurement tool. They measure light; specifically infrared light. Darker skin absorbs more light. If the devices were not designed and calibrated appropriately for patients with darker skin, they can give bad readings. This is something that could have, and should have, been accounted for in the design of these devices, but this was apparently not considered by engineers.
This is a big problem, and I am communicating it partly for the benefit of anyone with dark skin who reads this newsletter. Also, though, I believe it speaks to a potential contributing factor to the outsize mortality of COVID-19 in people of color. The devices that are being used to monitor a vital sign have an implicit racial bias that is documented here clearly.
When people say systemic racism is a problem in medicine, this is an example of what they mean. The issue of skin pigmentation was not adequately considered in the design of these devices, and when the device is a vital medical monitoring tool, that can be deadly.

What am I doing to cope with the pandemic? This:
A rather German meal to wrap up Chanuka
One of the traditions of Chanuka is to eat foods cooked in oil. As you might have noticed during the lead-up to Thanksgiving, I recently found myself the proud owner of a meaningful quantity of duck fat.
Last night, I used it to make latkes, a traditional potato pancake eaten by many Jews on the holiday. Latkes alone aren’t a very balanced meal, though. Traditionally they’re served with condiments like apple sauce or sour cream, but since these were made with duck fat, sour cream wasn’t an option within kosher rules. So instead, I decided to lean on German cuisine and serve up some sausages, with mustard and sauerkraut, to go along with the latkes.
This was super easy to do, and worked out really well. I recommend getting live-culture sauerkraut, which is way better than that fake vinegar-cured stuff.


Reader JG left the following comment on a newsletter from earlier this week:
I have read that 1.3% of NYC COVID cases have come from restaurants. Why are we shutting down indoor dining if it accounts for such a small percentage when we could go after more dangerous activities?
This is a good question, though I’m not sure it’s fully accurate in its particulars. It’s in reference to the following:
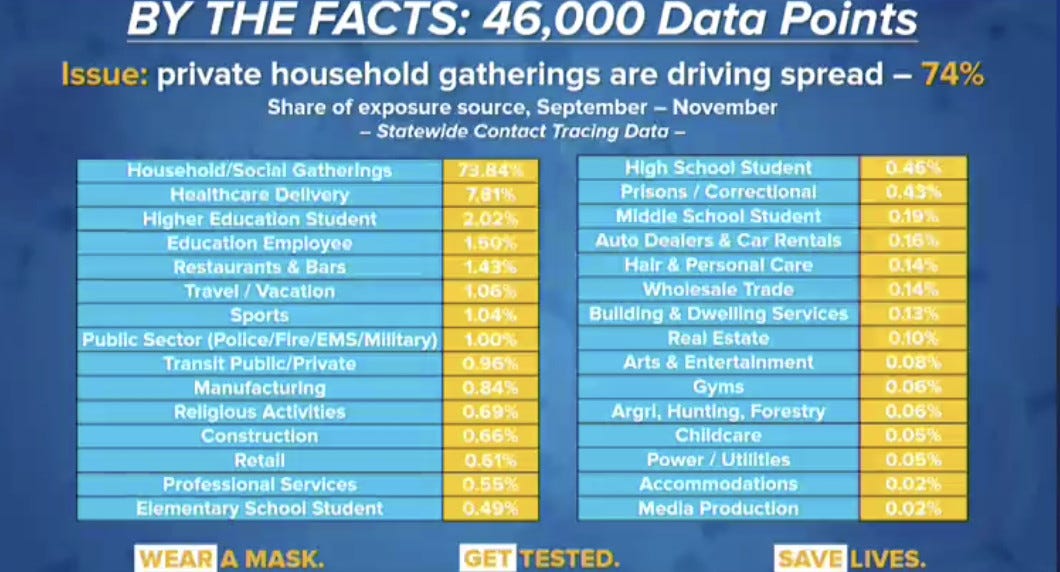
As we can see here, Restaurants and Bars statewide have been the source of 1.43% of cases over the last 3 months, and almost 74% of cases have been acquired at household social gatherings. That’s alarming. There’s a lot of other information to be obtained here—for example, it appears that gyms really are quite low-risk in New York, at least.
I responded to this question without these data at hand, but I wanted to provide them. Either way, here is my reply, which I still consider valid:
Well, firstly, these are the cases that we have information about; not everyone gets followup with contact tracers. Second, we have to assume that a substantial portion of people are not being honest with themselves or with contact tracers about the risks they have taken or what their potential exposure was. Based on those two things, I would anticipate that anything with a substantial signal of cases in contact tracing data is a potential issue. Being over 1% of total cases, to me, is substantial.
Lastly, I have to reject the premise that "we could go after more dangerous activities." Right now something like 74% of NYC cases are resulting from private gatherings at homes. I don't think these can be gone after. At this stage, these are almost certainly cases from Thanksgiving and other holiday gatherings. That distorts the signal but is also very difficult to police.
At this point any reduction in cases is worthwhile, to blunt the momentum of this thing. Closing indoor dining--which, in my opinion, was never appropriate to have open--is one of the few tools that are available.
Something interesting to me here is that education employees appear to be about as frequent a source of infections as restaurants and bars. In past issues, I had suggested that I think that indoor dining should have closed before schools in New York. Having seen these data, I now think that perhaps both should have been closed at the same time. Can’t argue with data.
You might have some questions or comments! Send them in. As several folks have figured out, you can also email me if you have a comment that you don’t want to share with the whole group.
I’ve been contemplating changing the schedule of this newsletter a little bit; perhaps reducing it from daily to 3 times a week. I’m interested in your thoughts; feel free to comment publicly or send them my way privately.
Thank you to those who answered me about this already; I’m taking all of the feedback under consideration.
Join the conversation, and what you say will impact what I talk about in the next issue.
Also, let me know any other thoughts you might have about the newsletter. I’d like to make sure you’re getting what you want out of this.

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
Correction: A reader pointed out that earlier this week, while I highlighted differences in the efficacy of the Moderna vaccine based on age, I went on to say that “There were also no apparent differences in efficacy across age, race, and sex of the patients.” This was just a mistake on my part; the sentence has been corrected to read, “There were also no apparent differences in efficacy across race and sex of the patients.”
Nice catch on the part of the reader who pointed this out! I didn’t get permission to name them here before press time, so they will remain anonymous but have my gratitude for this correction.
See you all next time.
Always,
JS
A newsletter 3 times a week still sounds great! I’m amazed at how many words you write every day!
You wrote, "Something interesting to me here is that education employees appear to be about as frequent a source of infections as restaurants and bars. In past issues, I had suggested that I think that indoor dining should have closed before schools in New York. Having seen these data, I now think that perhaps both should have been closed at the same time. Can’t argue with data."
Can I argue with your reasoning? Priorities matter. Schools are *more important* than eating in badwording restaurants, and for that reason could and should be allowed to remain open even when they represent some risk, even when indoor dining is forbidden.