

COVID Transmissions for 2-4-2022
A potential way that SARS-CoV-2 knocks out sense of smell; plus new vaccine efficacy data

Greetings from an undisclosed location in my apartment. Welcome to COVID Transmissions.
It has been 780 days since the first documented human case of COVID-19. I’m a little stunned to see how big that number has become. In 780, Charlemagne’s campaign to subdue Saxony is still in full swing, and he begins forced Christian conversions of subjugated Saxons.
Today, we’re going to talk about subjugation of the sense of smell by SARS-CoV-2. An interesting mechanism paper in hamsters has shed some light on how this happens.
Also, new CDC data reinforce the case for boosters in a world with Omicron and Delta.
Ongoing subscription offer:
THANK YOU to everyone who subscribed using this offer since last issue. The numbers are up, and I hope if they continue to rise I can outrank the misinfo newsletters that are ahead of me!
I’ve added some weekly paid content to the newsletter, and am running a subscription offer. Here’s the short explanation—the fuller explanation is in
This newsletter is the #5 result for “covid” on Substack
There are newsletters ahead of it that contain substantial misinformation
Part of the reason it is not the #1 result is that I have made a lot of content free, and Substack cares about how many paid subscribers you have, not how many total subscribers
I am pretty annoyed to be ranked behind misinformation newsletters, and I want to fix that. Which means I need to encourage and reward paid subscription, and I’m adding a paid-only weekly section discussing more general virology. However, I also believe strongly that essential COVID-19 information should be free, so everything related to COVID-19 in this newsletter will still be free. I’m also doing a 50% discount on new paid annual subscriptions until the end of February.
The offer can be found here:
Bolded terms are linked to the running newsletter glossary.
Keep COVID Transmissions growing by sharing it! Share the newsletter, not the virus. I rely on you to help spread good information, which you can do with this button:
Now, let’s talk COVID.

A potential mechanism for loss of the sense of smell in COVID-19
A recent virological mechanism paper in the journal Cell has proposed a mechanism for why some people lose their sense of smell with COVID-19: https://www.cell.com/cell/fulltext/S0092-8674(22)00135-0#.Yfp39sRryEA.twitter
This is a good paper in terms of its detective work, and it proposes a solution to one of the key problems with loss of the sense of smell in COVID-19: olfactory sensory neurons (OSNs), the cells that make you able to smell, do not really have receptors for SARS-CoV-2. OSNs are only infrequently infected with the virus, but anosmia is a frequent system.
In this work, the authors used a golden hamster COVID-19 model, which apparently models anosmia well, using actual SARS-CoV-2 infection. This is still an animal model, but it is nice to see that actual infection with the real pathogen in question was being done here.
The authors supposed that infection of nearby cells in the olfactory tissue might lead to cell signaling changes that could impact OSNs in a “non cell-autonomous” fashion. this phrase means that the effect caused by infection in one cell leads to an effect in a different cell. A signal is transmitted from the original infected cell that affects OSNs and causes them to shut down expression of olfactory receptors. Sense of smell is temporarily lost.
The way they figured this out is covered in this neat little cartoon:
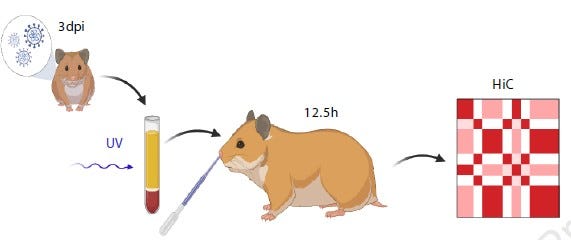
Here they have the hypothesis that whatever shuts down the sense of smell in COVID-19 is a signaling molecule that is produced in the infected host, but that is not related to the virus. They took sera from infected hamsters, inactivated all of the virus present, and then exposed uninfected hamsters. Whatever causes the loss of sense of smell, if their hypothesis was correct, should still be present and active in the serum samples. And indeed it was—they observed negative impacts on the expression of olfactory receptors.
The work presents an intriguing possibility for the mechanism of loss of sense of smell in SARS-CoV-2. Read the full paper for more details.
Update to CDC protection data now includes more Omicron infections
Recently I shared some CDC data that included infections though 12/15/2021 to examine vaccine effectiveness. In that issue I mentioned that these data probably did not contain many Omicron variant infections, so it was hard to generalize from the then-dominant Delta variant to the Omicron variant.
Well, thankfully, the CDC has now released an additional work that looks at follow-up including more Omicron variant infections: https://www.cdc.gov/mmwr/volumes/71/wr/mm7104e2.htm?campaign_id=9
This has allowed comparison of vaccinated and unvaccinated individuals during the Delta and Omicron variant periods in a meaningful way, against various outcomes. Here is how it shakes out:
Vaccine effectiveness (VE) against infection was estimated at 93% vs Delta and 80% vs Omicron for fully-vaccinated individuals who had also received subsequent booster doses.
VE against infection was estimated at 75% vs Delta and 64% vs Omicron for fully-vaccinated individuals who had not received a subsequent booster dose
From this we can confirm that Omicron is certainly more able to evade vaccination than Delta is, which is no big surprise but good to confirm. We can also determine that getting boosted does, indeed, provide added protection against infection. Great news! I guess the message here so far is to get boosted.
The authors also looked at VE vs death, but at the point analyzed, the death data were not mature for Omicron. So, this set only includes Delta. Still, this is a place where the results actually surprised me a little:
VE against death was estimated at 92% for unboosted vaccinated individuals and 98% for boosted vaccinated individuals
Now, look, that gain of 6 percentage points may look small. It may even not be real; I am not sure what the error on the estimates is. But the fact that there is a difference at all is somewhat surprising to me. The two doses from the initial vaccination are still very protective, but the addition of a booster may be offering a 6% gain? I would honestly say that that is worth it, especially considering the overall drop in protection against infection seen in the earlier part of the dataset, vs Omicron. It seems even more likely to me that in the near time, while Omicron is still predominant, it is meaningfully protective to get vaccinated.

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
Correction: last issue, I left in some text that mistakenly referred to a paywall. All of the content in the last issue was free. I removed the reference to a paywall in the online edition.

What am I doing to cope with the pandemic? This:
4-month vaccinations
We took our daughter to the pediatrician this week for her 4 month scheduled vaccinations!
These are, mostly, second doses of vaccine series that she has already started. Solidifying her protection against important childhood diseases is great!
There was a time when half of children did not survive to adulthood. I am very glad my child was not born during that time, and vaccines are part of the reason things have changed.

Carl Fink shared some updated data about the BA.2 subvariant, from the UK, which I found interesting:
I'm starting to see BA.2 hysteria in the popular media. It's odd, since the first wave of publicity was over a week ago.
A report from the UK says that BA.2, interestingly, is less able to avoid existing vaccine-induced immunity than Omicron BA.1: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1050721/Vaccine-surveillance-report-week-4.pdf
The report notes that with a full vaccine series and a booster, VE vs BA.1 and BA.2 was as follows:
This increased to 63% (63-64%) for BA.1 and 70% (58-79%) for BA.2 at 2 weeks following a booster vaccine.
The 95% confidence intervals here overlap, but the effectiveness is numerically higher against BA.2. These CIs are probably so wide because of a relatively small number of BA.2 cases in the dataset. I expect they will tighten up as more cases appear and we will have a better sense of things. Something to watch.
You might have some questions or comments! Join the conversation, and what you say will impact what I talk about in the next issue. You can also email me if you have a comment that you don’t want to share with the whole group, or if you are unable to comment due to the paywall in today’s issue.
If you liked today’s issue, please consider becoming a paid subscriber and/or sharing this newsletter with everyone you know.
Always,
JS
I wonder if this proposed mechanism for loss of smell, if correct, can give us any insight into potential therapies? While for a large majority of sufferers it does seem to recover eventually, it can in some cases take months. There are far more concerning post-COVID health problems, of course; nevertheless, it is something that seriously impacts people's mental health and quality of life.
I'm not fond of representing UV light as a spermatozoon, like the drawing you incorporated. (I'm pretty sure you didn't draw it yourself.)
About the boosting thing, though ... I got my third shot in October, and it's February. According to some sources, I am now very much less protected than I was in November. We can't actually know that until, say, May when numbers for February have actually been analyzed, though, right?