


COVID Transmissions for 5-10-2022
Get vaccinated BEFORE getting infected

Greetings from an undisclosed location in my apartment. Welcome to COVID Transmissions.
It has been 885 days since the first documented human case of COVID-19. 885 was a fascinating year. Charles the Fat was Emperor, and Vikings besieged Paris by navigating hundreds of longships down the Seine. The same year, a Viking nicknamed The Sea King (a vassal of Charles) got wrapped up in a plot to overthrow the Emperor. There was a lot going on! That siege of Paris, by the way, was fictionalized in the TV series Vikings. Emphasis on “fictionalized.”
It might be a stretch to connect this with the waters of the Seine, but today I’m going to share with you a new tool for monitoring wastewater for SARS-CoV-2 variants.
We’re also going to discuss yet more evidence that you want to get vaccinated before getting infected, and you don’t want infection to be your first experience with SARS-CoV-2.
Things at work have me exceptionally busy. I am running a department that has three major functions, and I am only one moderately-functional person. I am hopeful that some staffing or other support can come my way soon, but the upshot of all this is that in the short run, I remain committed to once-weekly issues of COVID Transmissions but am not sure if I can write more frequently than that.
Bolded terms are linked to the running newsletter glossary.
Keep COVID Transmissions growing by sharing it! Share the newsletter, not the virus. I rely on you to help spread good information, which you can do with this button:
Now, let’s talk COVID.

It’s better to be vaccinated first and get infected second
I’ve shared research to this effect before, but once again there is a study demonstrating that a person will typically experience an immune advantage if their first experience with SARS-CoV-2 antigens comes from a vaccine rather than from the virus itself. A short paper in Nature looked at vaccinated and unvaccinated who got infected with the Omicron variant of the virus, and observed that in the vaccinated group, infection with the Omicron variant served as a booster of sorts, and in fact appeared to expand the breadth of the immune response to different variants—including the Delta variant.
Overall, the unvaccinated people who were infected with the Omicron variant (BA.1 subvariant lineage) had:
2.2-fold lower BA.1 neutralization, 12.0-fold lower Delta neutralization, 9.6-fold lower Beta variant neutralization, 17.9-fold lower ancestral virus neutralization, and 4.8-fold lower Omicron sub-lineage BA.2 neutralization relative to vaccinated,
In every regard, having been vaccinated before becoming infected conferred an advantage in this small study. The vaccines are out there, providing benefits for those who have the wisdom to take them!
You can read the full paper here: https://www.nature.com/articles/s41586-022-04830-x
FDA wastewater surveillance project
I’ve just learned that the FDA has created a dashboard for identification of COVID-19 variants in wastewater. This is nice to see because it has been rather difficult to obtain good, centralized wastewater surveillance information for the US throughout the pandemic.
Wastewater has been a really good source of forewarning about the rise of new variants. The US continues to have really limited wastewater surveillance, but what we do have has been informative and provided good insight into what may be coming around the corner.
This new dashboard is available here: https://www.fda.gov/food/whole-genome-sequencing-wgs-program/wastewater-surveillance-sars-cov-2-variants
The tool generates this neat little graphic (it’s interactive over at the link):
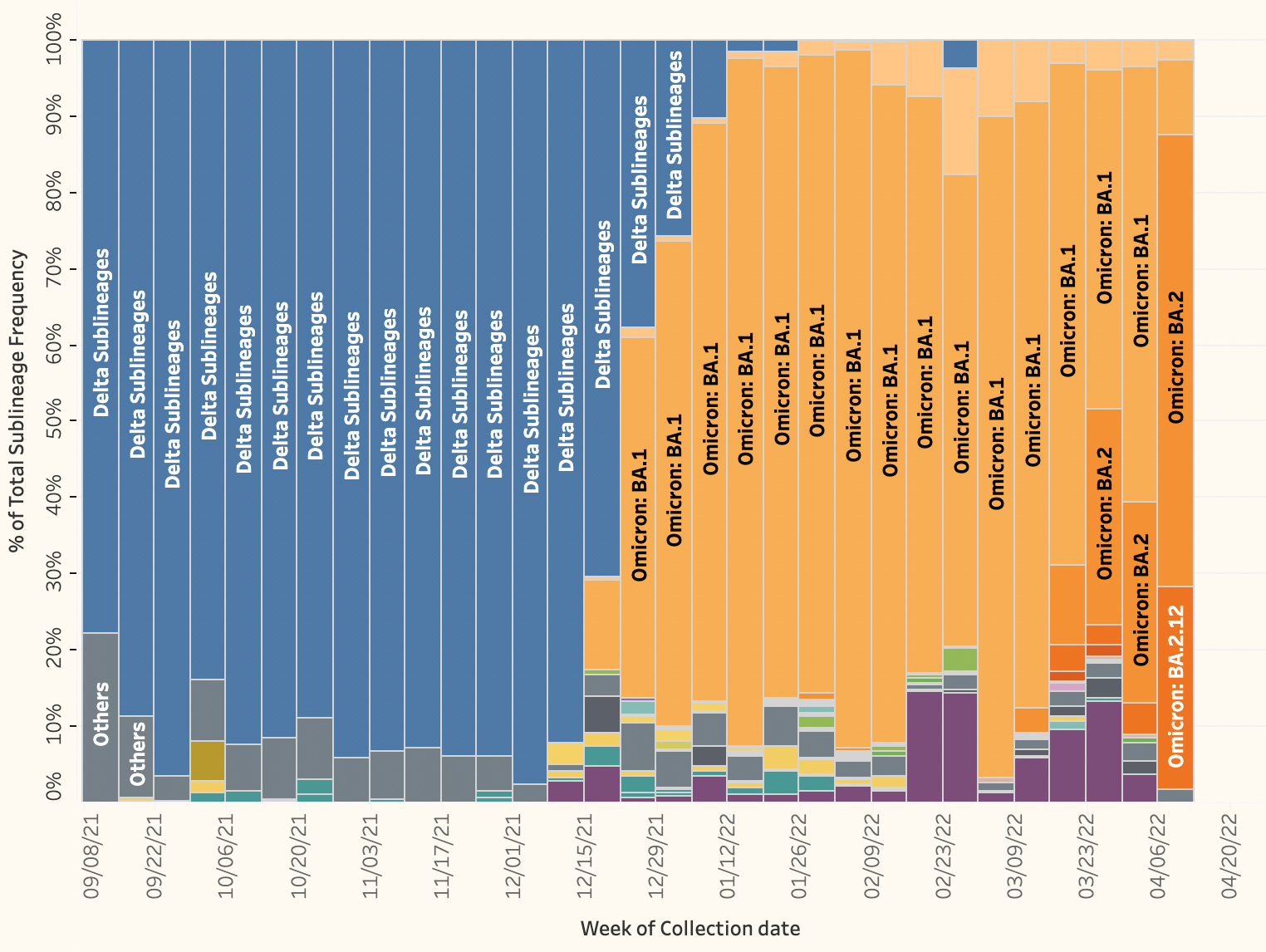
There’s a lot of information in the interactive version. Check it out!
At some point, I need to collate the various COVID-19 surveillance tools that I’ve recommended over the course of the pandemic. There are some really neat things that people have made, and they’ve been spread out over many issues. If some intrepid reader wants to help gather them into one place, let me know!

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.

What am I doing to cope with the pandemic? This:
Planning my first air travel since 2019
I booked a trip to San Diego today! I will be going there for a scientific conference that my company has some presentations at. I’m the lead for our medical congress presence and activities, so I wanted to be on site to see how our best-laid plans play out in the real world.
I’ll be wearing an N95 mask as much as possible during my journey. I may be three-dose vaccinated as well as recovered from an Omicron variant infection, but that doesn’t mean I’m not careful. Even if I wouldn’t get sick, I have an infant at home who I’d like to protect. And I don’t think the risk to me is entirely zero, either.

Reader Brock updated us on their experience in a clinical trial for an Omicron-specific vaccine:
In further news on my participation in the Pfizer omicron-specific trial, at my three-month visit last week following my booster that was either the omicron vaccine or the original, I was unblinded, and offered another booster, which was definitely the omicron-specific vaccine. I had been in the control group, and had received the original vaccine. I'll be giving them some more blood tomorrow, one week after my omicron-specific booster. This is the first time they've wanted blood so soon after the shot. Previously, it has always been one-month after the shot. The staff mentioned that there are a bunch of sub-studies they're keeping track of.
It’s very interesting to hear that the omicron-specific booster was offered to participants in the control arm after their unblinding! This could mean one of two things. First, the trial may be using a “crossover” long-term safety extension, where control group patients who completed the efficacy portion of the trial are offered the experimental vaccine on an open-label basis to see if there are any unexpected safety effects. This is a pretty common design approach for clinical trials.
Alternatively, it’s possible the trial designers are very excited by their early data and are convinced the specific vaccine works excellently, so they are offering it to control participants for ethical reasons—you don’t withhold a treatment that you know works. That’s just speculation. It could be either reason.
Special thanks to Brock for sharing these experiences!
Anyway, here in this trial, the subjects are clearly being treated with greater respect. They presumably enrolled in order to get access to this new vaccine, ideally, and the trial is designed to offer it to them when it’s appropriate. Glad to hear that this approach has been taken.
You might have some questions or comments! Join the conversation, and what you say will impact what I talk about in the next issue. You can also email me if you have a comment that you don’t want to share with the whole group, or if you are unable to comment due to a paywall.
If you liked today’s issue, please consider becoming a paid subscriber and/or sharing this newsletter with everyone you know.
Please know that I deeply appreciate having you as readers, and I’m very glad that if we must be on this pandemic journey, at least we’re on it together.
Always,
JS
Since, like yourself, I got COVID-19 after three doses of vaccine, I'm also encouraged to read about the synergistic immunity. (I just coined that phrase. I want credit!)
I do wonder if the study you cite said anything about duration of the immunity. For example, my current plan is to get a fourth shot (I'm over 50) before Worldcon in September. Will I need it by then?
Speaking of which, any chance you'll be in Chicago?
Dr. Skylar, I'm glad I found your substack!
I'm wondering if the results of the Omicron clinical trial are available online?
What were they looking for in the blood test?
Do you know if they were testing for troponin or d-dimer?