


COVID Transmissions for 7-14-2021
More on the third Pfizer dose, Pfizer in pregnancy, and J&J safety

Greetings from an undisclosed location in my apartment. Welcome to COVID Transmissions.
It has been 605 days since the first documented human case of COVID-19. In 605, the Chinese emperor Yangdi instituted the world’s first civil service examination system, beginning a long tradition of meritocracy that has expanded to many other nations.
Measuring things and making decisions based on those measurements is also a cornerstone of science, and today we’ll apply that to COVID-19 by discussing where new data are available—in the safety of the Johnson and Johnson vaccine and in the use of the Pfizer vaccine in pregnancy. And we’ll also talk about a topic where data are sadly lacking for now—in Pfizer’s claim that a third vaccine dose may be necessary.
Today’s issue is the last issue of the first year of COVID Transmissions, which began on 7/15/2020. Friday’s issue will mark the first one of the second year. It’s been a long journey and I’ve glad you’ve joined me on it. I hope that we continue to have good news in this second year.
Bolded terms are linked to the running newsletter glossary.
Keep COVID Transmissions growing by sharing it! Share the newsletter, not the virus. I love talking about science and explaining important concepts in human health, but I rely on all of you to grow the audience for this, which you can do by using this button here:
Now, let’s talk COVID.

More information about Pfizer’s claims regarding an additional booster dose
Pfizer has really put itself in the hot seat with claims that an additional dose will be required to combat waning immunity. Since the original announcement, many have asked for evidence, including the US federal government.
One thing that is apparent is that Pfizer’s attitude here is based on data from Israel, which has become a central source for population-based real-world data on their vaccine. The study that I shared recently, where vaccine efficacy against disease had dropped to 64%, supposedly, in the face of the emerging Delta (B.1.617.2) variant, appears to be at the center of these concerns.
The claim that Pfizer has made is that immunity begins to wane after about six months postvaccination. In the time since they made this claim, it has been realized that the only patients with follow-up that long will be either healthcare workers (a small population relatively speaking) or older patients. This may be a key piece of the puzzle here; if indeed immunity begins to wane after six months—and please note again we are talking about nearly total protection from severe disease still being in place—then it seems likely it is because of declining immune systems in older patients.
Interestingly, Israel has also begun giving third doses to patients who have compromised immune systems, another population that might be more likely to see declining immunity.
These developments suggest to me that Pfizer’s sweeping claim of need for a third dose was probably an overstatement of what the evidence is likely to say. That said, I don’t know for certain because I haven’t seen it yet.
I could believe that in older people and people with compromised immune systems, an additional booster is wise. I’ve been hearing speculation towards that idea for some months now. Patients and their healthcare providers have had access to tests that can confirm their successful antibody responses to vaccination, and it has been evident that in certain patient populations with immunocompromise, two doses just haven’t been enough.
However, that does not mean that three doses will be enough either, and it also doesn’t give me anything to go on to say that a third dose is necessary in patients who did have a solid response to two doses previously. Again, we’re in a vacuum of data here.
Interestingly, not everyone is in this data vacuum. Today, Pfizer shared some of their findings with the US government. Following that meeting, the Department of Health and Human Services issued a statement saying that Americans who have received two doses do not at this time need a third shot. The CDC and FDA issued a joint statement—something rather rare—saying the same thing. Whatever the data were, they don’t seem to have changed anything in the immediate future. I’ll continue to update on this as it develops.
The New York Times has coverage of this here, with some expert opinion: https://www.nytimes.com/2021/07/12/us/politics/pfizer-booster-shots.html
Guillan-Barre Syndrome warning added to Johnson and Johnson vaccine
The US FDA has added a warning for the neurological condition Guillan-Barre Syndrome (GBS) to the labeling of the Johnson and Johnson vaccine. In 12.8 million vaccinations, there were 100 cases of GBS, with 95 hospitalizations and 1 death. Incidentally, about 1 in 12.1 million people becomes an astronaut. So those are the odds we are dealing with here. Notably, all cases of GBS happened within 42 days of vaccine administration—this is typical for GBS onset. So, after about 6 weeks, it is unlikely that new GBS symptoms are vaccine-related. The reason I phrase it that way is that GBS is caused by more than just the Johnson and Johnson vaccine, as you might have imagined from the fact that the condition has a name.
GBS is a rare neurological disorder that most often happens in patients recovering from infections, including COVID-19. For example, here is a case report of a patient who had GBS associated with COVID-19: https://pubmed.ncbi.nlm.nih.gov/34046865/
The Mayo Clinic has an extensive information sheet on GBS, which also lists COVID-19, among many other infections, as potential causes of the syndrome: https://www.mayoclinic.org/diseases-conditions/guillain-barre-syndrome/symptoms-causes/syc-20362793
In GBS, the immune system attacks the nerves, which can take several manifestations. It can manifest as a tingling sensation, potentially beginning in the extremities, but can also involve difficulty walking, swallowing, or controlling bodily functions. these are things to watch out for if you have received this vaccine, but again, I’ll note they are very rare with vaccination. I would recommend also looking out for these things if you have had COVID-19.
GBS also happens with some other vaccines (still rarely), including the influenza virus vaccine. It is something to be generally aware of, despite the low chance of it occurring.
Pfizer vaccine efficacy in pregnant women, courtesy of Israeli real-world data
Now on to some better news. We have some efficacy data for the Pfizer vaccine in pregnant women, out of Israel. Unlike the study I shared last time, which used the term “pregnant persons,” this study uses the language “pregnant women,” so I will do the same here in order to not over-generalize the conclusions. However, this comes from a place of wanting to be accurate to my source material, much as I may be disappointed at the apparent lack of recognition of, or perhaps lack of inclusion of, trans patients in this study.
This was published in JAMA: https://jamanetwork.com/journals/jama/fullarticle/2782047
Here, the authors report a “hazard ratio” of 0.22 for documented SARS-CoV-2 infection in vaccinated vs unvaccinated pregnant women, a result which was adjusted mathematically for different pregnancy circumstances:
parity, population subgroup, trimester, prior children, influenza vaccine, obesity, infertility, and age
I have to say that this is pretty unusual. Vaccine effectiveness is usually a straightforward calculation. Here’s how the CDC describes it:
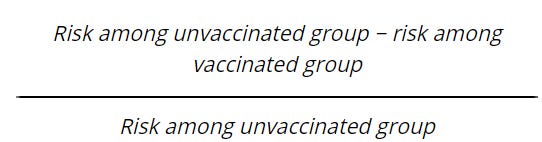
In this study, the reported adjusted hazard ratio, derived using much fancier statistics, was used to estimate vaccine effectiveness. This would give a 78% effectiveness, with a confidence interval between 89% and 57%. That’s pretty all right, though it does seem a bit lower than what we’ve seen in clinical trials…except that this study used a different primary endpoint from those clinical trials. It looked at confirmed SARS-CoV-2 infection (not disease) in the 28 days after the first vaccine dose. Pfizer first and second doses are administered 3 weeks apart, so this looked at confirmed infections starting 7 days after the second dose. In the clinical trials, the endpoint was confirmed COVID-19 (this means disease, not just infection!) starting 28 days after the first dose as well. The key difference here is, of course, that disease was not necessary to be included in the primary endpoint in this study in pregnant women. That alone may explain why the efficacy looks to have been a bit lower; in fact, only 89% of the patients in this study had documented symptoms.
We can compare the adjusted hazard ratio with what the more traditional calculation would have shown. The authors also provided the risk of infection in the vaccinated and unvaccinated groups, 0.33% and 1.64%, respectively. That allows us to roughly calculated vaccine effectiveness by the traditional method, too. That yields a 79.9% vaccine effectiveness against infection—again, not disease—vs the 78% that the adjusted hazard ratio indicated. I’m reassured that the numbers are this close together. You don’t want to see that adjustments of any kind of have caused huge swings in results.
On to safety. There were 68 patients who experienced adverse events. None were severe and all lasted for less than one day. Additionally the authors note that in an exploratory analysis of pregnancy outcomes, there did not appear to be any differences between vaccinated and unvaccinated patients.
All in all this paints a picture of a highly effective vaccine in pregnant women, with very few if any negative experiences reported. I’m very reassured by the totality of the evidence here, though I can’t say I was expecting any problems here. Still, you never know, until you have the data. And now with the data available, I feel confident that this vaccine is safe and effective in pregnant women.

What am I doing to cope with the pandemic? This:
Watching: Making It
“Making It” is a crafting-focused competition show hosted by Nick Offerman and Amy Poehler. It is extremely charming and I highly recommend it. Currently it’s in its third season.

You might have some questions or comments! Send them in. As several folks have figured out, you can also email me if you have a comment that you don’t want to share with the whole group.
Join the conversation, and what you say will impact what I talk about in the next issue.
Also, let me know any other thoughts you might have about the newsletter. I’d like to make sure you’re getting what you want out of this.

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.
See you all next time. And don’t forget to share the newsletter if you liked it.
Always,
JS