


COVID Transmissions for 7-27-2020
How long does immunity last?

Greetings from an undisclosed location in my apartment.
It has been 253 days since the first documented human case of COVID-19.
Housekeeping note:
I am working on some partnerships to improve the distribution, quality, and profile of the newsletter. I am open to suggestions on ideas for partners, so feel free to get in touch.
As has become usual, glossary terms are bolded words with links to the running newsletter glossary.
If you like what you see—or what you might see in the future—tell others about it so the newsletter continues to grow:
Now, let’s talk COVID.

It’s been a pretty quiet weekend for COVID news. The infection levels in the US are still terrible, and Florida is fast overtaking New York in terms of total cases. The situations in Brazil and Mexico also seem to remain bad, as well. I have heard that some of the western states in the US seem to be stabilizing in their case counts, but I’m a bit cautious about calling anything over until the drop holds for a couple of weeks.
Florida passes New York:
As reported here, the Johns Hopkins University tracker now has Florida with about 423,000 cases while they track New York at about 411,000: https://www.npr.org/sections/coronavirus-live-updates/2020/07/26/895596931/florida-case-count-surpasses-that-of-new-york-the-countrys-original-epicenter
If you’re in Florida, stay safe.
Duration of immune responses:
The in-depth is all about this today. But if you don’t believe me, listen to the NYTimes on this topic: https://www.nytimes.com/2020/07/26/health/coronvirus-antibody-tests.html

What am I doing to cope with the pandemic? This:
Reading

I finished Authority, the second novel in Jeff Vandermeer’s Southern Reach trilogy. It takes a shift from creepy-expedition adventure to creepy-spy adventure in this second book. I think it was a great read, with the author’s talent for character work expanding while he succeeds in keeping the mystery of his series both satisfying in its answers and puzzling in the new questions it poses. To a degree, this feels like reading a book about someone who is reading House of Leaves, but with deep existential stakes for what he takes away from it.
Watching
Weirdly enough we’ve been getting into Scottish comedies. We just finished Chewin’ the Fat, a sketch show that has a surprising number of well-done Star Trek (and particularly Deep Space Nine) sketches, and are now into its spinoff about Scottish pensioners (aka retirees here in the US), Still Game. While the former is crude, hysterical, and at times extremely outdated and cringey, the latter is really quite charming (though still at times cringey).

How long does protection last?
As the race to a vaccine heats up, the big questions are all about the nature of protection and immunity to COVID-19. Last week we discussed what understanding and evidence for the idea of protection at all—I happen to believe that there is good evidence to suggest humans should become protected against the disease.
The best evidence so far, of course, is that we do not see large amounts of reinfection around the world. The patients who are getting infected, with some limited and very unproven exceptions, are new patients who have never had the virus before.
This does not necessarily mean that any immunity is long-lived, however. Human coronaviruses, which can cause cold-type illnesses, usually do not bring about a durable immune response. This is part of the reason that we can get colds again, and again, and again.
We do not want a circumstance where most people are able to get COVID-19 again, and again, and again—this would really hurt disease control and any potential eradication efforts. At the same time, we don’t know much about the mechanisms of immunity to COVID-19.
Lately, a lot of headlines have focused on the possibility that antibodies may disappear rapidly after the resolution of infection with SARS-CoV-2. There were a few papers that made this suggestion, though the most recent was a letter to the editor titled “Rapid Decay of Anti–SARS-CoV-2 Antibodies in Persons with Mild Covid-19” and ran in The New England Journal of Medicine (NEJM). The following figure was provided as evidence of “rapid decay”:

Image is a graph showing log-scale decay in individual patients with mild cases of COVID-19, from day 0 (symptom onset) to day 120. The lines on this graph are all over the place, though some do drop by a couple of orders of magnitude over time. Some go up a little bit. Image adapted from NEJM.I hardly see decay in this figure, let alone rapid decay. Some of the lines even increase over time! But in truth, the biggest problem with this letter is the use of the word “rapid.” The data do indicate an overall decay in antibody levels, reaching about half of peak levels roughly 73 days after infection. This isn’t as big a problem as it sounds, and we’ll get to why in a moment.
There have also been a few past papers that suggested decay in antibody levels. One of the popular ones that circulated won’t be discussed in this newsletter because it is not peer-reviewed and on reviewing it myself I felt there were serious methodological flaws; the reason I mention it is to note that even when the data look good, there may be reasons to be skeptical that don’t jump out from the data alone. In this case, the false-negative rate of common antibody tests may almost entirely account for the apparent decay in antibody levels. So much for that.
Another preprint had a forecast where a complete antibody decay was projected from a bunch of scattered data, and it didn’t look compelling at all. But this was also widely reported in the press without peer review.
However, another earlier paper from Nature Medicine did get full peer review and does appear to show some decay in antibody levels…in 37 patients. You can read it here: https://www.nature.com/articles/s41591-020-0965-6. As of last check, about 16 million people worldwide have gotten COVID-19. While it is somewhat concerning to see a decay in a sample of patients, this is not what we would call a “representative sample”; it just doesn’t have enough size to be a convincing stand-in for the full population of people who have caught the virus.
Last week, though, I tried to convince you that it’s possible for humans to be protected from COVID-19 on the basis of a small amount of data collected in monkeys. At the time, I said this wasn’t definitive because it was only in a small experiment in an animal model. What I said was that it generates support for the hypothesis that humans could be protected.
That means it’s not very fair of me to dismiss this paper from Nature Medicine so easily; perhaps it supports a hypothesis of rapid decay, too. Instead, I’d like to walk through what this all may mean. We now have at least four reports, two of them somewhat questionable, that suggest decay in antibody levels over time.
My take on this is: this is completely normal.
If you open up any immunology text, you’ll eventually be greeted by a picture like this one:
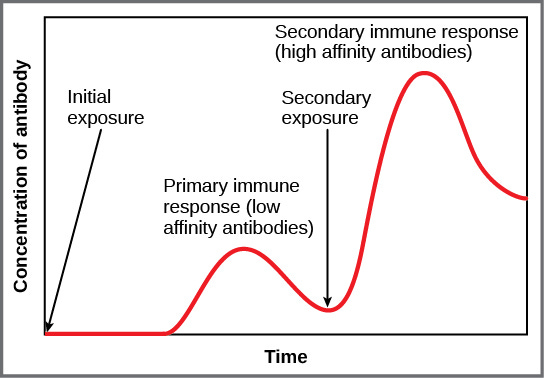
Image shows blood antibody concentration over time following two instances of infection; initial infection eventually leads to a high level of antibodies, which drop back down over time. A second exposure leads to an even larger spike, which eventually drops down again as well. Image from https://opentextbc.ca/biology/chapter/23-2-adaptive-immune-response/The fact is, we don’t make everything that our bodies can make all the time. It’s resource-expensive and it can throw our bodies’ balance out of whack. We make what we need, when we need it—at least under healthy conditions. And when you’re not infected with something, you don’t need the same level of antibodies circulating in your blood that you might need during infection.
Antibody levels drop down over time. It’s a fact of the way our bodies’ metabolism works. We make what we need, and if we need more of something, we make more of it. That’s why the second peak, after a second infection, is higher. It’s possible, also, for antibodies to fall below the level at which we can detect them, and then to jump back up on reinfection. Just because our tools cannot see them does not mean they are gone forever.
This is because we have immune memory cells, sitting dormant, ready to respond to new infections. These “memory B cells” are ready to produce huge amounts of antibody, and divide rapidly, at the earliest signs of a new infection. They will either make sure that the second infection is less severe, or that it never even takes hold at all. Also, when that second infection is done, the body holds on to more of what it needs to respond to future infections. The immune system has evolved to respond more strongly to things that are common in your environment and that you encounter frequently.
If we go back to that letter to the editor in NEJM mentioned before, we see antibody levels reducing by half every 73 days. That’s not at all outside of what we would expect for decay rates after an infection is resolved; it also means that levels drop to 1/4 after about 150 days. Even if that’s true, which we don’t have the followup to confirm, we don’t know if they continue to fall after that. Perhaps they reach a baseline low level, waiting to detect the infection again and resurge to protect the infected person.
At this point, however, I’m speculating based on what I know about immune responses and not bringing any other evidence to support the idea of longer-lived immunity to SARS-CoV-2. Part of the reason is that we have not lived with the virus long enough to know if what I’m saying is true; we do not have the follow up to know.
However, that doesn’t mean we’re without the ability to look for evidence. SARS-CoV-2 is very similar to its cousin, SARS-CoV-1. That virus, which killed a few thousand people, has been studied to a much greater extent and with much longer follow-up.
In 2007, a paper was published in Emerging Infectious Diseases that suggested that immunity to the first SARS virus could last at least 3 years: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2851497/
Another paper published in 2010 in Virology Journal also showed duration of antibody responses to SARS-CoV-1 for at least 3 years: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2988023/
Finally, in 2011, a paper in Journal of Immunology indicated that after 6 years, only about 8.7% of patients still had detectable antibodies against SARS-CoV-1: https://www.jimmunol.org/content/186/12/7264.long
Even if antibodies drop off after that, 3 years would be quite a long time. If we were able to create a vaccine that yielded immunity lasting that long, and got it widely adopted, we might be able to stop SARS-CoV-2 in its tracks.
The thing is, we don’t know that SARS-CoV-2 will behave the same way as its cousin. But we do know that it’s possible to generate antibodies, and we don’t have robust evidence at this time that the decreases in antibodies that we’ve seen so far translate to a loss of protection. What we do know is that a small drop in antibodies over time is rather normal, that similar viruses also see a drop in antibody levels, and that we have to keep an eye on this virus to see what time will tell.
For now, I don’t think that we’ve seen any compelling evidence for a loss of protection, at least. Despite several sustained hotspots around the world, we have only seen a handful of reports of suspected reinfection—and even then, these might be explained by bad tests, or if the data are correct, the rare weak immune response in a patient here or there. If, truly, immunity decays within months, we might expect to see many hundreds or even thousands of repeat infections.
As it stands, I’m optimistic that a durable immunity to SARS-CoV-2 is possible, and that with good vaccine design, we can get there. The data are still out, however, and this is a topic I will be keeping a close eye on. It’s a question that will inform a great deal about what our future world will look like.

Join the conversation, and what you say will impact what I talk about in the next issue.
Also, I welcome any feedback on structure and content. I want this to be as useful as possible, and I can only make that happen with constructive comments.
I want to thank reader Cheryl for some kind words on the last edition—I’m glad that this newsletter is helping to explain what’s going on with COVID-19 in an engaging and meaningful way.

This newsletter will contain mistakes. When you find them, tell me about them so that I can fix them. I would rather this newsletter be correct than protect my ego.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.
See you all tomorrow.
Always,
JS
You mention the possibility of eradicating the disease. Is that possible when it seems likely to have been transmitted from animals? We’re not going to be able to eliminate it among wild animals and we’re not going to vaccinate every human in earth. Right?
Is there some technical definition of “eradication” that addresses this?