


COVID Transmissions for 8-9-2021
How does the J&J vaccine perform against Delta?

Greetings from an undisclosed location in my apartment. Welcome to COVID Transmissions.
It has been 631 days since the first documented human case of COVID-19. In 631, the new viceroy of Egypt under the Byzantine Empire began a persecution of the Chalcedonian Coptic Church. It isn’t widely appreciated today, but in this era, Christianity was far from a unified monolith.
Today we’ll discuss new data about the J&J vaccine against the Delta variant, and a story about SARS-CoV-2 in deer.
Bolded terms are linked to the running newsletter glossary.
Keep COVID Transmissions growing by sharing it! Share the newsletter, not the virus. I love talking about science and explaining important concepts in human health, but I rely on all of you to grow the audience for this, which you can do by using this button here:
Now, let’s talk COVID.

Real-world data suggest that the Johnson and Johnson vaccine is effective against Delta variant
Real-world studies in healthcare professionals in South Africa suggest that the Johnson and Johnson vaccine is 71% effective against hospitalization due to the Delta variant, and 95% effective against death from that variant. The New York Times covers these results, which are still in preprint status: https://www.nytimes.com/2021/08/06/science/johnson-delta-vaccine-booster.html
Early on in the emergence of the Delta variant, we saw data out of the UK suggesting that a single dose of the AstraZeneca vaccine, which is very similar to the J&J vaccine in design, is not very effective against Delta. Two doses of that vaccine did appear to be effective against this variant, though.
So there has been a bit of a shadow hanging over the J&J vaccine as a result, with many thinking that it would require boosting in order to preserve efficacy against Delta. In these results, at least, that doesn’t appear to be the case. The vaccine seems quite effective, though the ability to prevent hospitalization is perhaps a little lower than we’d like.
These are the first data that give us a sense of how this single-dose vaccine performs with this variant, and they get us closer to an answer on whether it will need to be boosted—or replaced entirely. Looking at this, I think there’s the suggestion here that boosters won’t be needed for this vaccine. I’ll continue to monitor this.
SARS-CoV-2 in deer
Making the rounds recently is this paper from the USDA, suggesting that 40% of wild white-tailed deer in the US may have been exposed to SARS-CoV-2: https://www.biorxiv.org/content/10.1101/2021.07.29.454326v1.full.pdf+html
This is an interesting study; it looks, cleverly, at SARS-CoV-2 antibodies in white-tailed deer from historical samples before the pandemic as well as ones collected during the pandemic.
This helps control for something that is common in serological surveys: cross-reactive antibodies. Antibodies are generally very specific, for biological systems, but it’s that “for biological systems” that is important. Biology involves a lot of random processes, so sometimes, things are, well, sticky. Antibodies stick to things that they aren’t meant to stick to. Especially if those things are very similar to one another.
Imagine all of the mistakes that computers make at pattern recognition. There is a reason that humans can be differentiated from robots by picking out pictures containing certain features. Pattern recognition is hard, and antibodies are simple pattern-recognition machines. So, sometimes, they are “cross-reactive” against multiple things. This means that sometimes an antibody against one influenza virus might show up as having activity against another influenza virus—even if the person those antibodies came from never had an infection with that second influenza virus.
If we just went out and sampled random deer, we might find that there is high SARS-CoV-2 reactivity from antibodies in their blood, but we’d have no idea if this was because of infection with that virus, or some very similar coronavirus.
With the historical series here, we have a better sense of whether this is all due to some other deer-specific coronavirus. Take a look at this data figure:
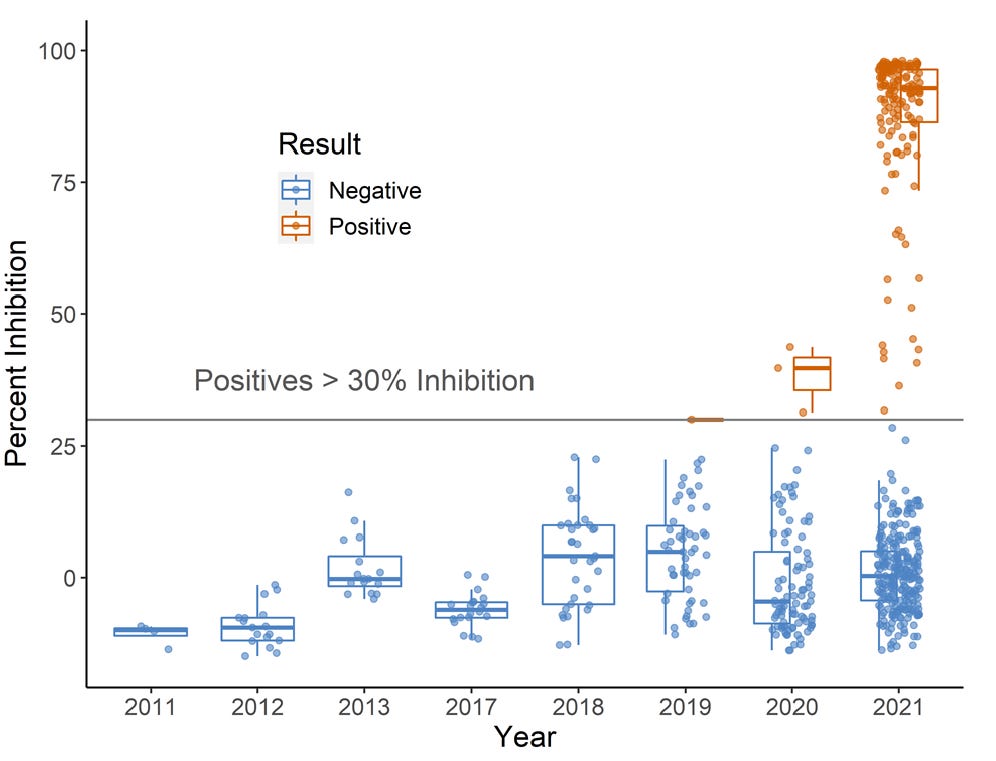
I think that the 2019 positive here is pretty marginal—there is a threshold for positivity and it’s right on the line. That’s probably some mild cross-reactivity. But the later results show a clear enrichment of antibodies that happens to correlate with the spread of the pandemic.
It seems to me, based on this, that SARS-CoV-2 found its way into deer. That’s not too surprising. Humans interact with plenty of deer, either in our back yards, in farms that collect them for meat, and through outdoorsy activities. On top of that, human-adjacent animals also interact with deer, and might themselves be able to be infected.
The bottom line of all this is that with the pandemic having spread, SARS-CoV-2 is now everywhere because humans are everywhere. Given the promiscuous nature of this virus in terms of what it is willing to infect, we find ourselves with a reality where SARS-CoV-2 probably never going away. If these results are the real deal, then it’s got animal reservoir potential that will allow it to return to human populations. What we can hope for is to control it—not to eradicate it.

What am I doing to cope with the pandemic? This:
Watching: The Pillars of the Earth
The Pillars of the Earth is a Ridley Scott-produced miniseries made in 2010, based on a book by Ken Follett. It has a cast that is better than what any miniseries deserves to have, including people like Eddie Redmayne, Hayley Atwell, Donald Sutherland, and more. The story focuses on a fictional town called Kingsbridge in England during the period of English history known as the Anarchy of King Stephen, which happened in the 12th century. King Stephen, a descendant of William the Conqueror, was locked in a bitter civil war with his cousin, Empress Mathilda, and this war was impacting the stability of England overall. The Pillars of the Earth edits the historical narrative a bit, but its still an interesting exploration of medieval personalities and intrigue. Also, it contains quite a few interesting finer points about the proper construction of churches. It’s a good series, and worth checking out.

Carl Fink asked me for a clarification on something I said last issue:
"The best that a booster can offer us is a restoration of effectiveness, gaining back about 10% efficacy."
Why do you say that? Have you seen a study indicating that? Because I see no obvious reason that it would not increase efficacy beyond the original two-dose regimen, especially if you change to a different vaccine for the booster. (There have been studies showing that using different first and second doses produces better antibody and t-cell response than two of the same agent.)
I agree with your conclusion, which I agree is obvious, but that one sentence puzzles me.
I could have explained this a little better. I was indeed making an assumption here, but I believe a reasonable one. My reply:
How much better than 95% effectiveness would you expect a booster to be able to achieve?
Imagine you're right, and the booster does produce better protection than the original 2-dose regimen. Then we have...96% effectiveness? 97? 98? That's still the same order of magnitude as 10%, and is a really small marginal gain.
I don't really need a study to demonstrate that vaccinating new individuals is going to be better than anything a booster can do, because the absolute best a booster could do is get people to 15% better protection. Can't do better than 100% effectiveness, after all--and I don't think any vaccine has ever been 100% effective anyway.
I do think boosters have value for certain smaller populations that are at substantial risk--immunosuppressed folks, for example--but as a population strategy they're a losing proposition and that can be demonstrated just through a thought experiment.
The conversation went a little further from there—feel free to look at last issue’s comment thread for it—with Carl pointing out that this is very specific for the situation we are in right now with this specific vaccine and the effectiveness drop we’ve seen against this particular virus variant. If the effectiveness drop were more extreme, my thought experiment here would not apply.
You might have some questions or comments! Send them in. As several folks have figured out, you can also email me if you have a comment that you don’t want to share with the whole group.
Join the conversation, and what you say will impact what I talk about in the next issue.
Also, let me know any other thoughts you might have about the newsletter. I’d like to make sure you’re getting what you want out of this.

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.
See you all next time. And don’t forget to share the newsletter if you liked it.
Always,
JS
You knew I would comment, right?
I'm just waiting for the result of the "two doses of Janssen" study that's in Phase 3 right now. Might it be as effective as Pfizer and Moderna? Moreso?