


COVID Transmissions for 12-24-2021
Two new drug EUAs; test accuracy vs Omicron; my COVID-19 experience

Greetings from an undisclosed location in my apartment. Welcome to COVID Transmissions.
It has been 738 days since the first documented human case of COVID-19. It has been two days since I became a human case of COVID-19.
This newsletter is going to look a little different today, because I am sick. The items that you read here will be a little shorter. Pandemic Life will be a bit different…but then I also think this is an important issue to read.
A couple of stories at the top about tests and new drug authorizations. Also, some reader comments.
Look, if you’re worried—I’m OK, and I want you to have happy, safe holidays. Merry Christmas to those of you who celebrate it. Shabbat Shalom, or just a really great Saturday to those who don’t.
Bolded terms are linked to the running newsletter glossary.
Keep COVID Transmissions growing by sharing it! Share the newsletter, not the virus. I rely on you to help spread good information, which you can do with this button:
Now, let’s talk COVID.

Some tests do not necessarily work against the Omicron variant
There has been an important update from the FDA on rapid tests for SARS-CoV-2. Dr. Amy Maxmen summarizes it well in this tweet, which also links the story:


Dr. Maxmen is an excellent journalist and a recommended follow from me.
The reason for the differences is dependent upon the way that these tests work. Some target parts of the virus that are mutated in Omicron.
Thankfully, the BinaxNOW and Quidel rapid antigen tests, both of which I have been using, are still accurate.
PAXLOVID and molnupiravir both have received EUAs from the US FDA
Two new oral antivirals will soon become available for early treatment of COVID-19 (neither was offered to me, I’m afraid!).
We’ve discussed PAXLOVID and molnupiravir before, several times.1
The PAXLOVID EUA is here: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-oral-antiviral-treatment-covid-19
Interestingly, PAXLOVID is authorized in both adult and certain pediatric (12 and older) cases.
The molnupiravir EUA is here: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-additional-oral-antiviral-treatment-covid-19-certain
Molnupiravir, which posted lower efficacy numbers in its trial than PAXLOVID did in its trial, and has had some hypothetical safety questions raised, has been authorized under a more narrow indication, of the two drugs. This is out of caution, and the general principle that when you have something that works really well (PAXLOVID), you don’t necessarily need to take an Emergency-Use-Authorization kind of chance on something that doesn’t appear to work as well. Specifically, this sentence is included:
…and for whom alternative COVID-19 treatment options authorized by the FDA are not accessible or clinically appropriate.
I’m a little uncomfortable that apparently a cross-comparison between two different clinical trials was at the root of this decision to limit molnupiravir. Clinical trials are massive experiments with a lot of individual quirks in each trial; usually FDA itself demands a single, head-to-head trial to control for such quirks before cross-comparing. But that is under normal approval circumstances, and not EUA circumstances, which may be what is making the difference.

What am I doing to cope with the pandemic? This:
Testing positive for COVID-19
I hate to say it, but SARS-CoV-2 found an ACE2 receptor on one of my cells and I’m in the thick of it now, my friends.
I seem to have acquired my infection some time during or after Worldcon 2021. Part of why I wanted to go to Worldcon was to explore the idea that we were in a new normal for COVID-19 and we need to find a way forward with this disease. As readers will know I designed a careful approach to attendance that went above and beyond the protocols the con required, particularly by being vaccinated with three doses of an mRNA vaccine, using an N95 mask and not just any mask, and taking a rapid antigen test every day.
The fact is, the risk environment changed drastically after I left for the con; I now think we should all expect to become infected and prepare for it as best we can. This is detailed in the Twitter thread I’ll share later. But back to the story.
I continued to take rapid antigen tests after the convention because a scratchy throat developed on Sunday of the con. On Wednesday, the test I took was positive. Yesterday, it turned positive almost immediately on starting the 15-minute incubation period for the test. Here’s what the positive result looked like:
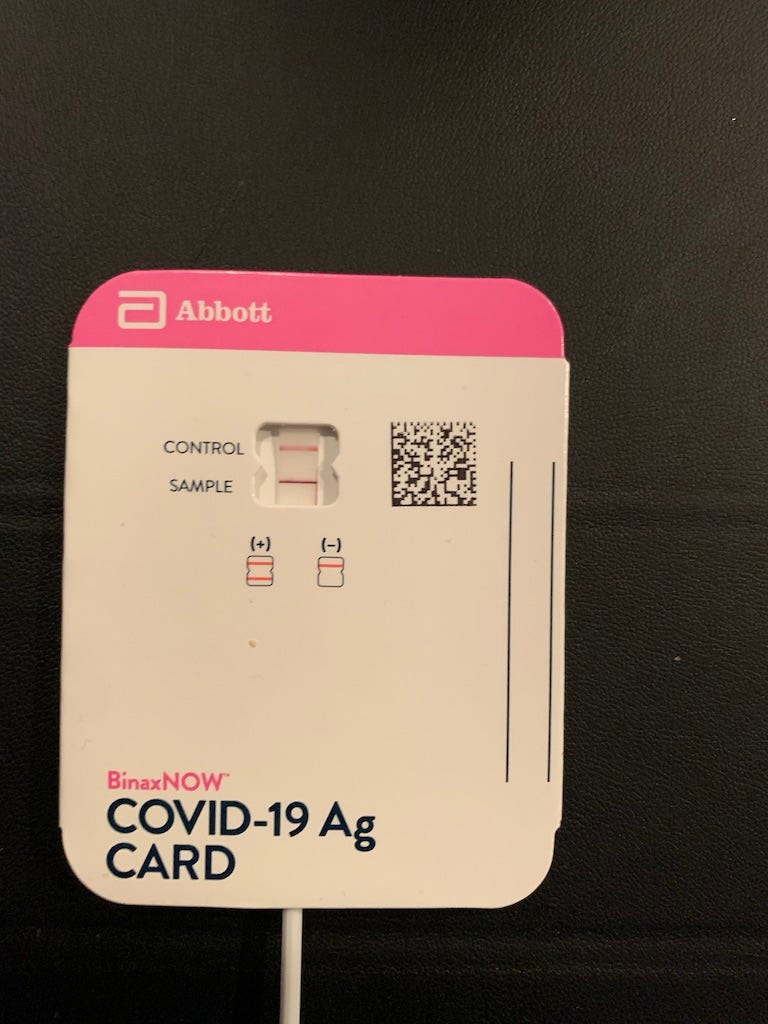
Thinking about having written an image description for that, I now wonder about accessibility issues with actually taking rapid tests. At the convention I spoke to someone about rapid tests who appeared to be blind or visually impaired, so I am curious about how that may work if anyone knows!
I’m keeping a record of my experiences with this case—one physician was kind enough to call it a “case history”—on Twitter. I will link that in a moment. But I wanted to call out specifically my reaction to seeing the red “sample” line:
That little red line meant that somehow a virus from a bat halfway around the world--a little blob of fat, water, protein, and RNA--had subverted me, a huge biological machine with extremely sophisticated weapons to fight off exactly this! It's hard to wrap the mind around.
Very strange feeling.
Overall, my case is thus far mild. The worst part of it is a completely killer sore throat. I have some congestion as well but it is not too noticeable. That throat soreness, though.
The mildness is a result of the mitigation measures I took; it may sound strange but even though I turned positive, all of my precautions worked. The point of these measures was to slow spread and lessen disease. I did not believe I could avoid this forever. My N95 kept me from spreading this to everyone I met. I know this because I met with people who did not test positive. My rapid testing helped me to break the transmission chain too, because I have isolated since getting it.2 Lastly, my vaccine doses have mitigated the severity. I have some risk factors! I have no doubt that this would be worse if I had not been 3x vaccinated. With two doses, I might be experiencing more of a flu-like illness than a heavy cold. With one or zero doses? I don’t even want to contemplate it.
Anyway, if you are interested in following my case, here is the Twitter thread where I am keeping a running log of my experiences and interpretations of them—you can click through for the full thing:


Noah writes, regarding the mechanism of TTS discussed last time:
PF4 antibodies are also implicated in HITT (heparin induced thrombocytopenia and thrombosis, a particular rare adverse reaction to heparin), so that's interesting. Also fully agreed that boosters should be incorporated into the definition of "fully vaccinated".
My reply:
The big question with HITT is...what's activating the T cell partner that lets the B cells proliferate? There must be some immune insult. Is it, perhaps in some cases, infection with a circulating adenovirus? There is some interesting science to be done here, and impactful too.
Nanotetrahedron wrote in to ask about reference sequences:
Question: each variant is described in terms of a series of mutations, but what’s the reference sequence the mutations are relative to?
My reply:
Nice question! These mutations are in reference to a "canonical" sequence isolated in Wuhan, originally called "Wuhan seafood market pneumonia virus" but now called "hCoV-19/Wuhan/Hu-1/2019". The overall lineage this is a part of is called 19A.
Here is the NCBI reference sequence: https://www.ncbi.nlm.nih.gov/nuccore/1798174254
And here is the same sequence on Nextstrain, an excellent resource for evolutionary virology: https://nextstrain.org/ncov/gisaid/global?s=hCoV-19/Wuhan/Hu-1/2019
IdahoFred wrote in with a message I don’t agree with, but which I am hearing too much—that if the vaccine doesn’t prevent infection, what good is it? Well, most vaccines don’t prevent infection. What they’re meant to do is keep you from getting seriously injured or killed by a disease. Here’s the exchange…
IdahoFred:
Maybe over a year ago my friend’s teenage son came home from school with Covid. He infected his brother, mother and father. No one was hospitalized and they all recovered. Later they all got the first two vaccine shots. Then the mother got the third. The other day I had a social lunch planned with my friend. He called to tell me that maybe we should cancel it. One of the sons came home with Covid and infected his brother and mother. My friend the dad had not been infected yet. As I have not been vaccinated and don’t intend to be I agreed that we should cancel our lunch. The vaccines seen useless to me.
My reply:
It sounds like everyone in this family is alive despite multiple exposures to and infections with COVID-19.
People who are unvaccinated die at approximately 10 times the rate as people who are vaccinated. Source: https://ourworldindata.org/grapher/united-states-rates-of-covid-19-deaths-by-vaccination-status?country=~All+ages
I would not call a product that reduces the chance of death by 90% "useless," unless I didn't particularly value my life.
Look, I hope to be very much living proof of this soon. I am infected, but I am doing OK. This is because I am vaccinated. The choice is not vaccination or nothing. It is a choice between getting COVID-19 with the prior protection that a vaccine offers, or getting it without that protection.
I chose “with”, and I’m very happy not to have the alternative.
You might have some questions or comments! Join the conversation, and what you say will impact what I talk about in the next issue. You can also email me if you have a comment that you don’t want to share with the whole group.

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.
See you all next time. And don’t forget to share the newsletter if you liked it.
Always,
JS

Contactless delivery is a lifesaver—for the delivery person. Literally. It saves lives. People ordering food in shouldn’t be allowed to turn it off.
Feel better, man!
As for those rapid tests: the two antigen tests listed should both detect SARS-CoV-2. The three genetic tests listed (Meridian, Tide, Applied DNA) probably do not. As the FDA acknowledges, these were not tested on actual patient samples and the results are preliminary.
So, how useful is the rapid test I'm literally going to take after I hit "Post"? I have no way to know, because it's OraSure's IntelliSwab test. However, if the two other antigen tests still probably work, I'm at least cautiously encouraged.
Note for the peanut gallery: I'm one of the people who was exposed to our host. So far, no symptoms and negative test. Mind you, I was also wearing a high-quality filter mask. (I was exposed to another known case maskless, but with social distancing--we ate dinner together. That's one reason I'm quarantining until my PCR test result comes in, or 14 days since the last day of the convention. I can't even get PCR tested until a week from Sunday.)
John, sorry to hear you came down with COVID, but glad you're holding up well.