


COVID Transmissions for 12-27-2021
Omicron hypotheses and data

Greetings from an undisclosed location in my apartment. Welcome to COVID Transmissions.
It has been 741 days since the first documented human case of COVID-19. It has been five days since I became a human case of COVID-19.
Today’s issue tries to address many of the swirling and speculative claims about the Omicron variant. It is opinion-heavy, and there is some highly technical stuff, but I’m trying to get ahead of certain ideas that are spreading rapidly without clear and definitive findings supporting them.
Bolded terms are linked to the running newsletter glossary.
Keep COVID Transmissions growing by sharing it! Share the newsletter, not the virus. I rely on you to help spread good information, which you can do with this button:
Now, let’s talk COVID.

Roundup of things I am hearing about Omicron
I’ve been hearing a lot of speculation about the Omicron variant’s features and behavior, and I wanted to just collect and evaluate them in one place. We are still at a place where we have more questions than we have answers with regard to this variant, so this isn’t a piece where you should assume anything here is true.
For a lot of this, I will be drawing on supporting evidence found in Public Health England’s Technical Briefing #33, which is found here: https://www.gov.uk/government/publications/investigation-of-sars-cov-2-variants-technical-briefings
CLAIM: the Omicron variant evades vaccine-induced immunity and can make a vaccinated person sick
I have intentionally worded this claim in a way that I don’t like, to make a point that blanket statements are always misleading.1
At this time, I can say that Omicron variant viruses have a number of immune-evasion mutations. UK data indicate that the Omicron variant is more likely to cause disease in patients who have received only 2 doses of a vaccine, and that this likelihood increases the longer-ago that person received their vaccine. However, this effect could still be partly because the first people to receive vaccinations were the most at-risk populations.
Still, I think it is clear that the Omicron variant is able to cause disease in vaccinated people to a greater degree than past variants. I can’t put a number on it, but I think if you’ve only had 1 dose of an adenovirus-based vaccine or only 2 doses of an mRNA vaccine, you should consider yourself susceptible to disease until you hear otherwise.
The picture for those who have received an additional dose of either of these options is less clear. 2 doses of an adenovirus-based vaccine look only weakly protective, if protective at all, against disease. 3 doses of an mRNA vaccine offer some protection against symptomatic disease, but this protection appears to wane over time, bottoming out around 10 weeks after the third dose. See here:

The SpikeVax/mRNA-1273 (Moderna) vaccine with only 2 doses has the same pattern that we see for the Comirnaty/BNT162b2 (Pfizer) vaccine above:
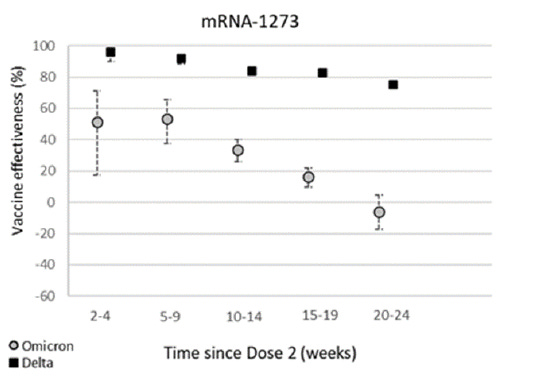
So here, in the UK at least, we definitely see some weakening of vaccine effectiveness, particularly with only 2 doses.
In my opinion, this is happening because these vaccines were not designed to combat a variant like Omicron. We are swamping them with antibodies by using boosters, but that protection is transient. If we want to restore protection against disease, it is going to take an Omicron-specific vaccine, in my opinion. However, if Omicron just causes a mild cold-like illness in vaccinated people, I am not sure how much that vaccine will be worth the costs to deploy. We will have to see how it bears out.
Still, bottom line, I think everyone should consider themselves susceptible to disease from the Omicron variant. Vaccinated people, especially ones with more doses, will be meaningfully less likely to die or experience other serious complications when they become infected. The dynamics of the pandemic have, certainly, changed.
CLAIM: Omicron variant infections are less likely to lead to hospitalizations
This is hard to tease apart from the reality that right now, infections in general are less likely to lead to hospitalizations than earlier in the pandemic. More people are vaccinated in more countries where Omicron surges are present, and more options to boost available vaccines have created populations with high levels of antibodies. The antibodies in question are particularly good at preventing hospitalization, as I understand things to work, so we have improved background protection in the population at large.
At the same time, the rate of hospitalization due to Omicron in the UK is down about 60-70% relative to what would have been expected from Delta data. Some portion of that effect may be due to vaccines and some portion may be due to something inherent to the virus. The relative contribution of each is unclear at this time.
CLAIM: the Omicron variant has a shorter incubation period
There is some evidence that Omicron variant infections have a shorter incubation period until disease is apparent. However, I think these data are very early and incubation periods are always a range. Something to keep in mind is that with vaccinated people being so much greater a share of the population, you have more people out there with antibodies whose immune systems may react a bit faster to the presence of an Omicron variant infection. It is hard to tell if the inherent kinetics of the infection are really different or not, at this time. It is also hard to estimate any specific timing for the incubation period.
I rate this one at a “maybe.”
CLAIM: the Omicron variant has changes that make it less able to infect lower respiratory tract cells, and thus it causes more of an upper respiratory disease
To understand this one, we have to do a quick review of SARS-CoV-2 entry. In this section I am going to mention a lot of esoteric protein names. When reading these, try not to focus too much on the names themselves. They are just characters in a story. They have weird names, but the important part is how the characters interact and where.
SARS-CoV-2 entry can follow two pathways. Both begin with attachment of the virus spike protein to a cell surface protein called ACE2. Then, the virion is either taken into the cell in a little pouch called an endosome, or it can fuse directly to the cell. The latter option requires the virion to be processed by an enzyme called TMPRSS2, a “protease” (protein-digesting enzyme). TMPRSS2 cuts the spike protein in a way that exposes the “fusion peptide.” The fusion peptide is a part of the spike protein that makes the virus’s envelope membrane fuse with the cell membrane, allowing the virus genome to be released into the cell.
In the endosomal pathway, the virion is cleaved by a totally different protease named Cathepsin L. This exposes the fusion peptide too, but the virion fuses with the endosome membrane instead.
Basically, the TMPRSS2 pathway allows fusion at the outer surface of the cell, and the Cathepsin L pathway happens inside a little bag that is brought into the cell.
There is this hypothesis running around that the Omicron variant has more trouble entering cells that express TMPRSS2. Instead, Omicron variant viruses, the hypothesis says, have to go into the endosome and use Cathepsin L. Since TMPRSS2 is found in cells deep in the lung, this hypothesis claims, Omicron has trouble infecting these cells. This is supported by some experimental evidence: https://pubmed.ncbi.nlm.nih.gov/34951565/
This leads to less-severe disease, supposedly.
This sounds reasonable as a hypothesis,2 but I think it is a long way from bearing out as a definitive explanation. An equally compatible hypothesis is that Omicron variant infections are not spreading deep into the lungs of vaccinated people, because in the lower respiratory tract there is better access to the IgG antibodies that the mRNA vaccines produce so efficiently. Or, it is a combination of these two options.
My point is that while this is a nice and interesting idea, we are going to need a lot more evidence supporting it before it can be said to explain anything observed with the Omicron variant.
Overall
I would say we can be confident that you will have better protection against Omicron, if briefly, by getting an mRNA vaccine booster. An unvaccinated person is certainly not as well-protected as a vaccinated person, particularly against hospitalization.
However, vaccinated people should be prepared to experience a mild illness until Omicron-specific vaccines can be generated.
I think this is an event that has been anticipated by virologists for a while. Some time ago, I shared a paper showing that human common cold coronaviruses mutate to escape preexisting immunity gradually, making them potentially again competent to cause disease:

I said something in this issue that I think has aged fairly well:
Even if protection wanes a bit over time because of changes to the virus, we might have our immunity “updated” by circulating SARS-CoV-2 strains without experiencing severe disease. And, knowing that this can happen, we always have the opportunity to update the various vaccines.
Here were are 2 years into this pandemic, and a variant has emerged which begins to escape preexisting immunity. Perhaps this was a little faster than we might have expected, but the virus is still adapting to humans. Like with the human common cold coronaviruses, that escape is not total, and only a mild disease is likely. As vaccinated people gain immune experience with the Omicron variant, I expect they will expand their immune profile to be protected against it, and most of us will move on.
This doesn’t mean you should go out and try to get COVID-19 if you’re vaccinated, though. We should try to slow the massive increase in cases going on right now, so that the most severe cases are not sent into an overwhelmed healthcare system at once. We need to continue to take mitigation measures, but I do think we are taking a big step on our way to a fundamental change in our relationship with COVID-19.

What am I doing to cope with the pandemic? This:
Continuing to detail the experience of my mild COVID-19, and the science underlying it, on Twitter
As I reported last time, I am going through the science going on with my COVID-19 case, and the emotional and physical experiences of the case, on Twitter. I update this daily. Here’s a link to the beginning of the thread:

This project is consuming a lot of my time. Which is good, because I am in isolation.

There were a TON of good comments on the last issue. Too many for me to reproduce them all here. If you are interested, please go back and have a look. I think quite a few interesting things came out of those conversations.
You might have some questions or comments! Join the conversation, and what you say will impact what I talk about in the next issue. You can also email me if you have a comment that you don’t want to share with the whole group.

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.
See you all next time. And don’t forget to share the newsletter if you liked it.
Always,
JS
Yes, I made a blanket statement about the invalidity of blanket statements.
I’ve heard of things like this happening with other respiratory viruses as well—for example, in influenza viruses, where a preference for different sorts of sialic acid receptors can change whether or not a virus species can efficiently infect and transmit in different parts of the human respiratory tract. More on that here: https://www.virology.ws/2009/05/05/influenza-virus-attachment-to-cells-role-of-different-sialic-acids/
I'm so sorry you have COVID!
Last issue you said you no longer thought cloth masks were sufficient. Could you explain that a little more?
Relevant to the vaccine discussion -- first evidence that Omicron infection confers cross-immunity to Delta: https://twitter.com/sigallab/status/1475584463941914635. This suggests that perhaps that we wouldn't need a multi-valent vaccine to take on both Omicron and Delta. Scott Gottlieb had expressed the worry that it would be otherwise.
We still need to ask if it's really worth it to roll out a variant-specific vaccine, of course. But it should be pointed out that the primary endpoint of the original trials was prevention of symptomatic infection -- not just severe disease. Whether that goal now needs to change is a conversation scientists, government officials, and the public can have, but it won't do to just move the goalposts and hope no one notices.
That's not to suggest that preventing mild illness is *as important* as preventing hospitalization, or to diminish the hugely important role vaccination is still playing in saving people's lives. But it leaves a lot to be desired in terms of democratic accountability, not to mention respect for people's intelligence, to alter policy and messaging without even acknowledging that it is, in fact, being altered.