


COVID Transmissions for 12-8-2021
Omicron can evade immunity, but perhaps not as much as we fear

Greetings from an undisclosed location in my apartment. Welcome to COVID Transmissions.
It has been 752 days since the first documented human case of COVID-19. In 752, King Pepin the Short of France began a massive military campaign. Pepin, who won the throne in 751, was the first of the Carolingian dynasty. This lineage of kings replaced the Merovingians, who were believed to be descended from a sea monster, and ruled Frankish courts for centuries.
The replacement of the Merovingians with the Carolingians is a funny thing to be thinking about in a world where the Delta variant of SARS-CoV-2 may eventually be supplanted by the Omicron variant.
Today, I will share with you some of the first robust molecular data on immunity against the Omicron variant. It is incredible work that is made all the more amazing for the speed with which it was performed and disseminated to the world.
Bolded terms are linked to the running newsletter glossary.
Keep COVID Transmissions growing by sharing it! Share the newsletter, not the virus. I rely on you to help spread good information, which you can do with this button:
Now, let’s talk COVID.

Early data from South Africa about what Omicron actually does in the face of neutralizing antibodies to SARS-CoV-2
I’m very excited to report that there now exist some early data on the ability of vaccine-induced neutralizing antibodies to take down the Omicron variant of SARS-CoV-2. These data are so new that they are not actually on a preprint server, even, at the time that I write this. Instead, they are found on the website of a South African virology lab run by Dr. Alex Sigal: https://www.sigallab.net
Please note, the paper appears at this time to only show up if you visit the site on mobile. No idea why.
The Sigal lab has done something incredible here. These experiments are not easy to conduct, and the speed with which they have performed, analyzed, interpreted, and provided the manuscript to the world is stunning. Lives are potentially in the balance, and this lab has acted accordingly. I’d give them a medal if I could.
Several steps are involved in this paper:
Isolation of Omicron variant SARS-CoV-2 virus (this required collection from human subjects)1
Sequencing of genomes from this isolated virus to confirm that it is in fact Omicron variant
Selection of a population of (Pfizer) vaccinated individuals and collection of serum from them to test antibodies against Omicron; some were also previously-infected and then vaccinated
Performance of virus neutralization assays to determine how strongly serum from vaccinated people reacts to neutralize Omicron variant viruses
Performance of infection experiments with isolated virus in a human lung cell line, to determine whether Omicron variant viruses still use the ACE2 receptor
I’m going to skip right to the second to last bullet, because that’s the practical information, but I just want to underscore how involved—and cutting-edge—this work was. Really, the authors deserve a lot of credit.
Anyway, here are the results:
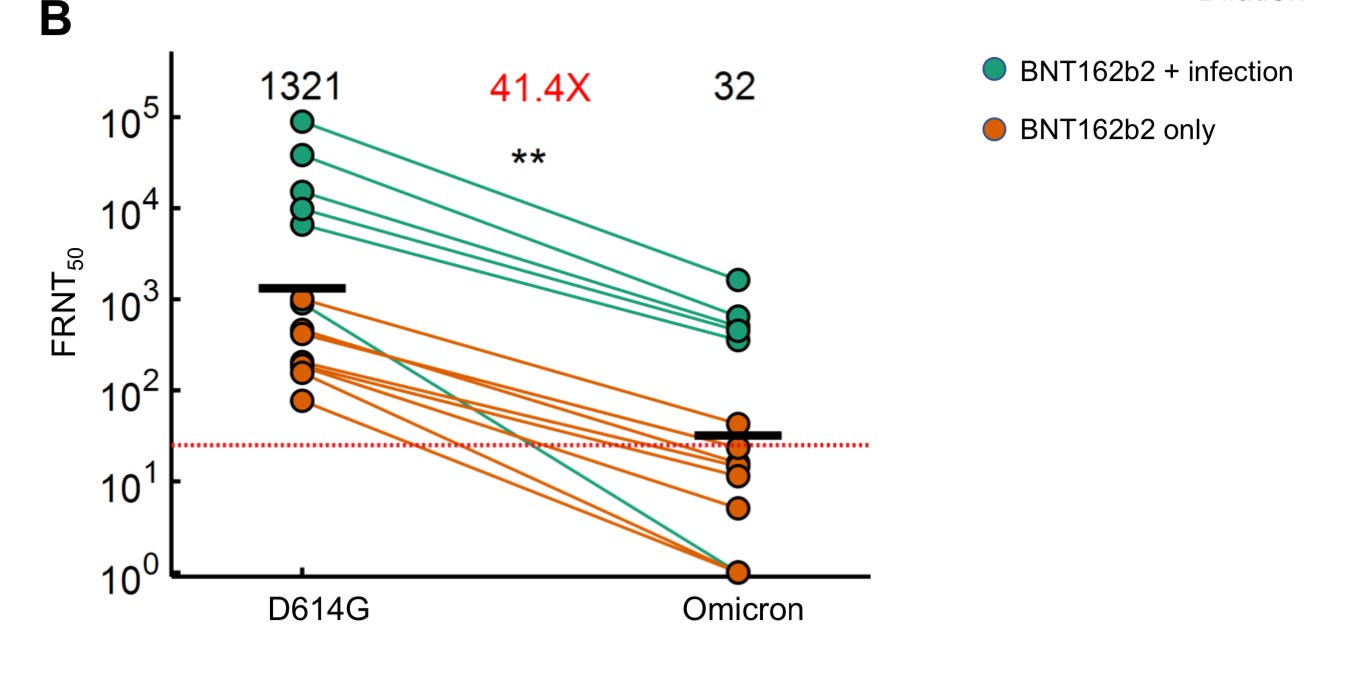
What we are looking at here is substantial evidence of escape by Omicron from vaccine-induced immunity. However, it is not all doom and gloom. Firstly, there were still some samples that did have around 100-fold dilution before they reached 50% neutralization of the Omicron variant, even with just vaccination. That’s not fantastic, but it’s better than nothing. Furthermore, the samples from patients with prior infection clearly had better ability to contend with the Omicron variant virus.
The prior-infection + vaccination samples do not, in my opinion, represent some unique population of people. They are a group that had higher levels of antibodies than the typical recipient of the Pfizer vaccine, because they had effectively been exposed to virus antigens three times in life rather than two. There are other groups who have higher levels of neutralizing antibodies. Research has demonstrated that people who received the Moderna vaccine have meaningfully higher levels of neutralizing antibodies than those who received the Pfizer vaccine. It is also known that boosting the Pfizer vaccine elevates antibody levels.
Another thing that elevates antibody levels is getting infected. People who have been vaccinated before start with a higher baseline of neutralizing antibodies before they become infected with Omicron, but in a real person rather than an experimental assay, the infection with this variant would prompt expansion of memory cell populations and new production of antibodies. There would be an immune response that would substantially increase the numbers of antibodies in these sera in a matter of days.
I think that, on a very preliminary basis, we can extrapolate from these findings to the idea that the vaccinated will still have protection from at least severe disease with the Omicron variant of SARS-CoV-2. This is not settled science, but I feel OK about this as a hypothesis. Boosted people will do even better, and may be able to avoid getting sick at all. SpikeVax (Moderna)-vaccinated folks may do better also. And, I think there’s a good case that people who were previously infected and then vaccinated will do well also.
The spectrum of disease that Omicron variant infections may cause in such people as I’ve just listed is not clear. Some will have no disease at all, others mild disease, and some (very few in my opinion) will get severe disease.
The work here is not without its limitations. First of all, they looked at 14 samples from 12 immune patients. This is not such a robust analysis; we would want hundreds or thousands of patients to feel confident of a representative sample. There are patient-variation factors that might introduce bias here. Perhaps all of these people had weaker immune systems than the average person; we don’t know. Next, like I mentioned, there are cells that divide and grow and enhance the immune response during actual infection. Those are not present here. Lastly, we have nothing here about T cells, which may have a role to play as well.
Still, this gives us an early picture. Yes, the Omicron variant contains immune escape features. No, I don’t think they compromise all the protections that vaccination can offer. I think a lot of people will still be protected, particularly from the worst outcomes. I am not seeing the end of the world in these data.
To move along to the other part of it, the authors asked a question of mechanistic interest for the study of this variant: does Omicron still use ACE2 as its receptor, or has it evolved to use something else?
To do this, they infected a human lung cell line that does not express ACE2 with their isolated Omicron variant virus particles. They compared this with infections conducted in the same cell line, but modified to express ACE2. They found marked differences in the ability of Omicron variant SARS-CoV-2 to infect cells with and without ACE2. ACE2 appeared to still be necessary for Omicron variant infection to take place. So, we can be reassured that the changes in the Omicron variant are not so extreme that the receptor for the virus has changed.
That’s also likely to be good news.
This paper is remarkable for the speed with which we have it and the value of the information at so early a time in the emergence of this new variant. This is no doubt going to inform health policy around the world, and other labs are going to look to confirm these findings as robustly as possible.
Science keeps stepping up its game to fight this emerging virus, and I’m very happy to see it.

What am I doing to cope with the pandemic? This:
Contemplating some diet changes
I’ve mentioned before that I’m on a fitness journey, and now I have very specific goals in mind. I read a piece by a nutritionist recently, who made the point that supplementation of protein is really important when you are trying to both lose weight and build muscle—and it makes sense, since the body will happily lose muscle weight as well as fat when you’re not taking in enough calories. I’m looking into it more deeply, but I think I might have to start a regimen of protein supplementation so that I can convince my body to focus on ditching fat and not muscle.
We’ll see how it works out!

Reader Sam commented on our story about myocarditis from last time:
The apparent paucity of vaccine-associated myocarditis cases among the 5-11 age group is really interesting. It also seems clear now, based on data presented to VRBPAC and ACIP (among other sources), that:
- The reaction is most common in males in their late teens and early 20s.
- It does occur following the first dose in a significant number of cases (though far less frequently than following the second).
- It's occurring less frequently with third doses, though that could just be due to selection bias.
- It seems to be somewhat more common with the Moderna vaccine than with the Pfizer vaccine.
I wonder if, taken together, this information can tell us anything about the underlying mechanism of mRNA vaccine-induced myocarditis?
I don’t know if this tells us anything. But I did ramble on about it in my reply anyway!
The last point is the most informative, IMO.
Point 1 is of course vital information but I don't think speaks to mechanism, or at least not in a way that's meaningful for me.
Point 2 I think is evidence that this is kind of a crapshoot, or that some amount of inflammatory load is required to get to this. It's also hard to read into because the case numbers for this event are pretty small.
Point 3...as you say. Hard to rely on that so far.
Point 4 tells us potentially that this is a dose-dependent effect. That's interesting on its own, and I think the most likely explanation.
But all we can really learn from that is that the effect, when it occurs, is probably a direct reaction to the vaccine rather than some sort of cascade that the vaccine kicks off but which then self-reinforces. Otherwise I would expect the context where it occurs to be more random. Point 2 may also speak to this; giving two doses in quick succession may provide enough dosage on average for some people to pass a threshold for inflammation and get myocarditis.
We still don't know, though, what makes it happen in the certain people where it happens. That's hard to assess.
I wonder, though, if this might be another situation where a longer dosing schedule could help. I also still think accidental intravenous delivery may be involved, or a contributing factor to at least some of the frequency.
It's hard to say for certain.
You might have some questions or comments! Join the conversation, and what you say will impact what I talk about in the next issue. You can also email me if you have a comment that you don’t want to share with the whole group.

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.
See you all next time. And don’t forget to share the newsletter if you liked it.
Always,
JS
There are still numerous conspiracy hucksters on the Internet who claim “SARS-CoV-2 has never been isolated.” For this reason, I like to point out whenever a lab group has independently isolated this virus. Here we have it happening again—and there are dozens of other groups that have done this kind of work. We know that this virus is the causative agent of COVID-19, and it has in fact been isolated many times.
There's been some question over whether the growth of Omicron vs. Delta is due to increased immune escape, increased intrinsic transmissibility, or both. I'm increasingly seeing commentators suggest that Omicron's performance so far suggests that it's at least as intrinsically transmissible as Delta, in addition to having considerable immune escape properties. Where do you land on this question?
Not directly about COVID-19, but you wrote, "I’ve mentioned before that I’m on a fitness journey, and now I have very specific goals in mind. I read a piece by a nutritionist recently, who made the point that supplementation of protein is really important when you are trying to both lose weight and build muscle—and it makes sense, since the body will happily lose muscle weight as well as fat when you’re not taking in enough calories."
With my particular mindset, I see "nutritionist" and think, "Person who didn't actually get licensed as a Registered Dietitian," since "nutritionist" is not a professional and licensed designation like "Professional Engineer" or "Licensed attorney." Is this person a nutrition researcher, a registered dietitian, or just someone who made a sign that says "Nutritionist"? Anyone can use that word about themselves, unlike, say, "Real Estate Inspector", which required a government license.