


COVID Transmissions for 2-11-2022
Intranasal vaccines, random sampling, and Omicron-specific boosters

Greetings from an undisclosed location in my apartment. Welcome to COVID Transmissions.
It has been 787 days since the first documented human case of COVID-19. The 787 is a beautiful aircraft, and I’ve loved the times I’ve gotten to be a passenger on one.
Today I’d like to start with a PSA: many places are rolling back mask requirements or other restrictions. I think in a lot of cases, this is premature, but not as premature as you might think. It does look like the Omicron wave has burned out in many locales. That has left us with low background transmission, and perhaps, with a period of relative safety for the time being. I do think it is reasonable to relax some restrictions as that trend continues, but please—pay attention not to what local politicians are saying, and rather to the local numbers. This isn’t over yet, much as I’d love for it to be.
As for what we’ll discuss today, we’ve got two vaccine stories—one about an intranasal vaccine, and one about an Omicron-specific booster—and a story about epidemiological technique.
Have a great weekend! If where you are is enjoying a lull in COVID-19, please do try and make the most of it as safely as you can.
Today’s issue is 100% free content.
Bolded terms are linked to the running newsletter glossary.
Ongoing subscription offer:
To encourage paid subscriptions—which will help me outrank misinformation newsletters, all too common on substack—I am running a 50% off deal for annual plans (through the end of February). A big thank you to those who have subscribed via this offer.
The offer can be found here:
So far this offer has been very successful, and we are 7 free subscriptions away from the next round multiple of 100 for total subscribers, and 10 paid subscriptions off from the next 100 for paid supporters. I think (hope, really—I’m not certain) it will be impactful on search ranking if we meet those thresholds. Thank you all! I think if we can break these thresholds, we’ll rank up vs some of the misinfo newsletters I’m in competition with.
Keep COVID Transmissions growing by sharing it! Share the newsletter, not the virus. I rely on you to help spread good information, which you can do with this button:
Now, let’s talk COVID.

Intranasal vaccine shows promise in mice
Something we’ve mentioned in this newsletter before is that there are antibodies which circulate in the blood, and these seem to correlate well with protection against severe disease…but there are also antibodies, called IgA, that are found in “mucosal surfaces,” the places where our cells meet the outside air. These antibodies, for many respiratory viruses, are a road to protection not just from disease, but from infection.
Naturally, we want to make IgA antibodies in response to COVID-19 vaccines. One strategy to do that would be intranasal vaccination.
An intranasal vaccine being worked on at Yale, in Dr. Akiko Iwasaki’s lab, has shown a great deal of promise in a preprint study: https://www.biorxiv.org/content/10.1101/2022.01.24.477597v1.full
One of the corresponding authors on this study, Dr. Benjamin Goldman-Israelow, was a graduate student at Mount Sinai when I was there as well. I say this partly for full disclosure but also to share how impressed I am with Ben and his career.
This work got picked up by the media in several places, including Rolling Stone (which I believe has misspelled Ben’s name): https://www.rollingstone.com/culture/culture-features/covid-19-vaccine-nasal-spray-no-needle-1296030/
In this work, they tried several different vaccination strategies, all of which began with administration of a non-intranasal mRNA vaccine “prime” followed by different boosting options. One option was the provision of spike protein intranasally to the mice, as depicted here:

I chose this particular experiment because it is representative of the work in the paper, but they did a lot more than this—including testing an intranasal mRNA vaccine.
Anyway, for the experiment I showed, one of the key readouts was weight loss over time. This is typical in mouse experiments in virology, because sick mice can lose a substantial amount of weight.1
Let’s look at the weight loss and survival results:
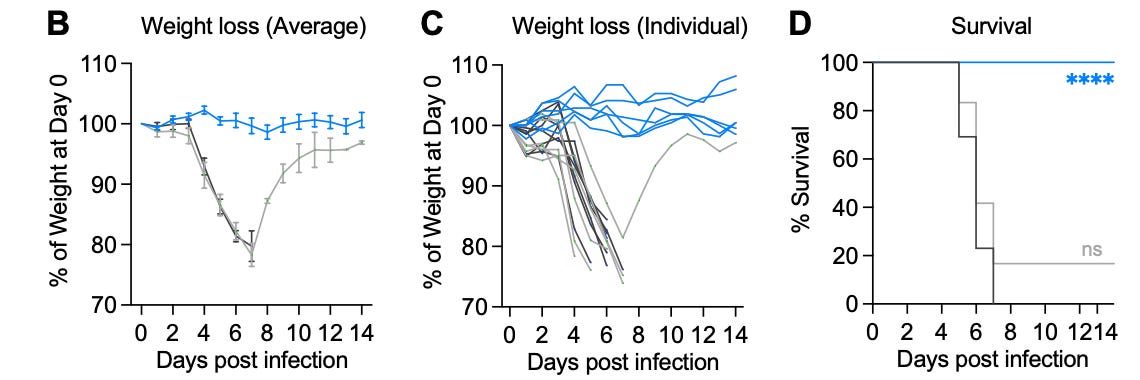
These are striking results; I would interpret them as the vaccinated, intranasally-boosted mice not getting sick at all. The dose of virus used here was enough to kill nearly all the other mice in the experiment. That’s really meaningful.
The intranasal vaccine mouse group also had lower amounts of virus RNA in their lungs, on average—a good sign for the prospect of reducing or eliminating infection.
There is a lot more work to be done here to indicate if this will work in humans, but this experiment appears to justify continued pursuit of that work. I hope it pans out!
The case for changing how we assess COVID-19 burden
There was an interesting persuasive piece by biostatistician Dr. Natalie Dean recently in Nature that argued for random sampling instead of aggregate, incidental testing, to assess how much COVID-19 we have in the community: https://www.nature.com/articles/d41586-022-00336-8
What did all of that lede mean? Well, right now, we count the number of positive tests that occur in a place, and that is scored as the count of cases in that place. As it turns out, this method misses a lot of cases, for a variety of reasons. Many people don’t test when they get sick. Others use home antigen tests that don’t get counted in official statistics. There are other problems as well—because the data are only representative of people who seek out testing, there is potential behavioral bias.
Ecologists, epidemiologists, and other math-driven biological researchers have long used random sampling to estimate various “true” population sizes. In this technique, a random representative group of individuals are counted, and then the results of that counting are extrapolated to the wider population. The random choice of individuals to test means that we are avoiding biases of test choice and reporting; the researcher recruits people before study outset, and randomly tests them on a routine basis.
It requires careful design, but the approach can get us a much better estimate of the true incidence of COVID-19 in the population. Read Dr. Dean’s argument on it. She’s the expert on this.
Moderna Omicron-specific vaccine results in monkeys
Carl Fink gets credit for calling my attention to this. Moderna and collaborators have released results of a study of an Omicron-specific booster in laboratory monkeys. I know I’ve mentioned Omicron-specific boosters as potentially important here before, so I wanted to share these results, but only after thinking about them for a while—they don’t go in the direction I was thinking they might.
Here is a preprint of the work: https://www.biorxiv.org/content/10.1101/2022.02.03.479037v1?s=08
The bottom line is that the Omicron-specific booster and the control (a booster specific to the ancestral lineage), appear to perform equally well against a virus challenge 2 weeks after booster administration. This included virus challenges with the Alpha, Beta, Delta, and Omicron variants.
Before we throw out the idea of using Omicron-specific boosters, however, I want to just point out some things:
We already knew that if you recently had an ancestral-lineage booster, it provides protective immunity in humans against the Omicron variant; I covered that here recently, a few times
We did not know if an Omicron-specific booster would elicit any protection against any variant, because one had never been tested before
The Moderna vaccine uses a higher dose of RNA compared to its competitors, and the booster version uses a lower dose of RNA than the prime dose version
Monkeys aren’t people
#4 is important for any animal study, so let’s not forget it. I’m glad that the Omicron-specific booster worked here at all, and I hope it performs at least as well in humans.
#3 I mention for one very specific reason: this study has got people worried about the concept of Original Antigenic Sin, where the initial response to one variant of a virus biases all later responses to that variant’s relatives. People think that original antigenic sin might be why the Omicron-specific booster didn’t perform better than the ancestral booster here. They may be correct, but I mention #3 in the event that they are correct—the phenomenon might be most pronounced because a very high prime dose against the ancestral variant is given with Moderna’s vaccine, followed by a lower boosting dose against the new variant. I would want to see equivalent data with the Pfizer vaccine, which I have not seen with my own eyes yet—I’ve only heard rumors.
Now, to #1 and #2. These are meant to be considered together. Since we already know that in humans, people who got an ancestral-lineage booster 2 weeks before exposure to Omicron are protected against Omicron, is it surprising that we see the same in monkeys? The issue that Omicron-specific boosters are supposed to correct is not the effectiveness of the booster at its earliest effective time, but rather the durability of the protective response. Right now it is thought that the ancestral-lineage boosters confer added protection against disease for only about 10 weeks after administration. What we really need is something that will be more durable than that.
Unfortunately, the researchers here did not do an experiment that would tell us if the Omicron-specific booster confers that added durability, because they only looked at performance 2 weeks after booster administration.
So, I’m not convinced, as some others appear to be, that this means those of us already vaccinated will get no added benefit from an Omicron-specific booster. Maybe that’s true, but I would prefer to see some data in humans that speak to the actual durability of the response before closing the book on this.
The authors do note that if Omicron has truly replaced other lineages, the variant-specific vaccine may be a better option in new vaccinees going forward. That too will require human studies to confirm.
Ultimately, my view that an Omicron-specific booster may work out well has taken a hit here with these results. I see reasons not to give up on it—and I’m encouraged by the fact that it doesn’t appear to underperform the older version—but it might turn out that this specific-booster strategy doesn’t work with regard to this particular variant.
That might be OK, though. Since the vaccines seem to protect extremely well against severe manifestations of Omicron variant-mediated disease, and may even prevent long-term symptoms on at least some level, I’d say they still work excellently. We’ve seen that in recent data, too—New York County, where I live, is 83% vaccinated. Here’s how it fared through the whole Omicron wave:

That is very, very different compared with March 2020. It’s far from perfect, but we certainly have the upper hand against this disease now—because of vaccines. Amidst worrisome news, I don’t want you to forget that.

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
No corrections since last issue.

What am I doing to cope with the pandemic? This:
Watching: 1883
I am a sucker for anything with Sam Elliott in it. That guy’s voice and acting are just so fun. So I got interested in the show 1883 before I knew it was a prequel to the show Yellowstone, and I have to say, I’ve been enjoying 1883 on its own. It’s basically a dramatization of the events that many folks simulated in the computer game The Oregon Trail, but substantially more vivid (with harsh, adult themes).
I’ve been pleasantly surprised, also, with the quality of the performances of Faith Hill and Tim McGraw, who are much better known as musicians than as actors.
I’m enjoying it, and I think it makes an effort to say something about the pioneering spirit. Also, having watched a couple episodes of Yellowstone, now, I have to say the two shows seem to have almost nothing to do with one another—except perhaps that some characters are distant descendants of those in 1883, and both shows involve cows, guns, and horses.

There was some interesting discussion on the last issue—not all of which I participated in. I encourage you to go back and read it. Selecting out one comment, Noah, who is an active healthcare provider, weighed in on test results:
Definitely agree with you on the topic of negative tests. I wouldn't even take a PCR test after a positive home test, but it's probably required for time off work, reporting, etc. Clinically though I'm pretty sure any single positive test is sufficient to isolate given the low false positive rate.
I have nothing to add, but I thought others might find this useful.
You might have some questions or comments! Join the conversation, and what you say will impact what I talk about in the next issue. You can also email me if you have a comment that you don’t want to share with the whole group, or if you are unable to comment due to a paywall.
If you liked today’s issue, please consider becoming a paid subscriber and/or sharing this newsletter with everyone you know.
Always,
JS
Compassionate guidelines set a requirement to euthanize mice that lose more than a certain percentage of their body weight; such mice are considered to have been killed by the virus they were infected with, for experimental purposes.
I am inviting you to speculate about something.
Many viruses (most famously HPV, but also the various hepatitis viruses that I can think off the top of my head, and maybe CMV) increase the risk of cancer in survivors.
Given that it seemingly affects so many body systems, what are the odds that SARS-CoV-2 infection will increase the probability of cancer years down the line? Obviously, we won't know the 10 year risk of even the early strains for at least another 8 years, but ....
Those intranasal vaccine results are really exciting. I hope the NIH and the Biden Administration are paying attention, and are thinking about ways they can help accelerate such research.
Regarding the Omicron booster, obviously we need to see the human data before drawing any strong conclusions. We'll likely get those data in a month or two. I wonder, though: might we expect the results to be different, whatever they ultimately are, if subjects are given, say, Novavax's (pending) Omicron-specific booster after priming with an mRNA vaccine?
Also, what exactly is the functional significance of the Moderna vaccine's higher dose? Does more mRNA mean more spike protein is produced following vaccination? Does it actually contain more than 3x more mRNA, or is it made up of proportionally more LNP? Even if not, do the different LNPs in the two mRNA vaccines have at effect on immunogenicity or reactogenicity?