


COVID Transmissions for 2-18-2022
Ancestors of the spike protein in bats; vaccination protection against Long COVID

Greetings from an undisclosed location in my apartment. Welcome to COVID Transmissions.
It has been 794 days since the first documented human case of COVID-19. In 794, Charlemagne abandoned his canal project to link the Rhine and the Danube, which would have had a tremendous impact on European history if he’d actually finished it.1
When it comes to COVID-19, I don’t think we should be giving up—even if it seems like the virus may have won a place in human ecology, we can still control it.
Today, we’ll discuss more analysis showing that vaccines, even taken after the infection, can fight Long COVID. We’ll also delve into some more work on the origins of SARS-CoV-2.
Have a great weekend!
Schedule note: Next week there is the Presidents’ Day holiday in the US, and I am also likely to be distracted by a family matter. There will be at least one issue next week, and I will aim for two, but the normal schedule will not be followed. We will return to the normal M/W/F schedule the week after next.
Today’s issue is 100% free content.
Bolded terms are linked to the running newsletter glossary.
Ongoing subscription offer:
To encourage paid subscriptions—which will help me outrank misinformation newsletters, all too common on substack—I am running a 50% off deal for annual plans (through the end of February). A big thank you to those who have subscribed via this offer, and to the large number of subscribers both free and paid who have signed up recently.
The offer can be found here:
So far this offer has been very successful, and we have now exceeded the next 100-subscriber milestone, and we’re just 3 paid subscriptions off from the next 100 for paid supporters. Thanks to that, we’re up to #3 in search results for “covid.” There is still one misinformation newsletter ahead of us. Having seen the impact of your support on my ranking, I’m now certain it will be impactful if we keep the numbers rising. Thank you all!
Keep COVID Transmissions growing by sharing it! Share the newsletter, not the virus. I rely on you to help spread good information, which you can do with this button:
Now, let’s talk COVID.

UK Health Security Agency: Vaccination halves risk of Long COVID
According to a UK Health Security Agency review of 8 studies, full vaccination against COVID-19 reduces the risk of Long COVID by half compared with one-dose vaccination or going totally unvaccinated.
This has been published in the BMJ: https://www.bmj.com/content/376/bmj.o407
This finding collects disparate evidence to continue to build a picture that vaccination can reduce the risk of long-term COVID symptoms, but a reduction by half is not as encouraging as one might hope. That said, long-term COVID symptoms are a wide range of things, and the studies examined here used different definitions of the condition. I would like to have a sense of the severity of symptoms as well; if vaccination can prevent the most impactful long-term symptoms, that is clearly better than if it cannot.
Another aspect of the work was a look at the effect of post-recovery vaccination. The authors again found improvement in Long COVID symptoms among patients who got COVID-19 vaccination after their recovery from COVID-19 compared with those who did not. I could not tell you exactly why such an effect would happen, but it is interesting—in a sense, it really is never too late to get some kind of protection from Long COVID, it would seem.
Now, I do want to emphasize that because these were observational studies and were not randomized, we can’t be totally certain that there weren’t behavioral differences between the groups that somehow impacted the results here. It doesn’t seem extremely likely to me, but I did want to highlight the potential limitation. There are other potential limitations with observational studies as well. The design is not as strict, and the data are often not as clean.
Still, I think there’s something here, considering that there was a large number of studies to be looked at, all showing an effect. That’s good news.
Detection of bat coronaviruses that readily infect human cells
One of the mysteries in understanding the origins of SARS-CoV-2 that has been with us since its emergence is the fact that it was quite divergent from its closest known ancestor. This meant it had some sequence features that were new, but we couldn’t point to where they came from. For example, it included features like a “furin cleavage site,” a site that allows its spike protein to be processed and readied for action by the host protein furin. It also meant that it had an enigmatic and previously unknown receptor binding domain in its spike protein, which was capable of binding with high affinity to the human ACE2 receptor, something its known (at the time) close bat virus relatives could not do.
Investigations into virus evolution and origins are hard; sometimes we never find out the exact answers. There are a lot of reasons for this, but one of them is that if you find something close enough to the emerging virus you were looking for, you might think it’s just a variant of that virus that spilled back into wherever you are looking. So we have to look for clues as to what general circulating populations a new virus might have come from.
Some weeks ago I shared a paper demonstrating that viruses circulating in bats already have the evolutionary foundation for a furin cleavage site, some being just one mutation away from gaining it.2 This gives us a clue that easily, the unexpected furin cleavage site in SARS-CoV-2 spike might have originated in bat populations.
Now we have another clue. Until now, there were no bat coronaviruses identified that readily bound to human ACE2 and entered human cells. Now, a publication in Nature demonstrates exactly that kind of virus: https://www.nature.com/articles/s41586-022-04532-4
They identified viruses in the wild (from bats in Laos) that had similar receptor binding domains to SARS-CoV-2, and then they did an experiment to see if the spike proteins from those wild viruses could enter human cells expressing human ACE2 to the same degree that SARS-CoV-2 can. Here’s the experiment:
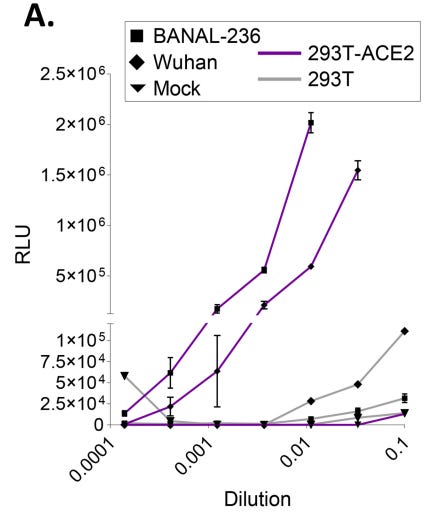
In this experiment, a fluorescent protein is used to create light when the pseudotyped virus successfully infects the cells in the experiment. We see with BANAL-236, the bat virus spike chosen for this experiment, that cells expressing human ACE2 are permissive to infection—the same as for their Wuhan SARS-CoV-2 control. In fact, the BANAL-236 spike looks like it might even be a little better at infecting human cells than SARS-CoV-2 spike.
So now we have found, in bats, the other enigmatic feature of SARS-CoV-2: a spike protein that can enter human cells using ACE2 as the receptor.
None of the viruses in this paper also had a furin cleavage site, but we now have seen both features present in wild-type coronaviruses that can be isolated from global bat populations. To produce a SARS-CoV-2-like virus, all that would need to happen is for viruses with a furin cleavage site to recombine with ones that have this receptor binding domain, in a bat somewhere…or potentially another animal that interacts with bats.
The very astute may be wondering how this is relevant to Wuhan, China when this paper was in bats in Laos and the one I covered previously was in European bats. It’s a good question, but it has what seems like a silly answer: bats are social animals that can fly. This combination means that viruses spread among them like a juicy rumor in a small town. A bat can range a great distance, and they interact with other individuals frequently. Bat viruses, therefore, can spread over long distances and find themselves in many other individuals.
Humans do the same thing—we’re social animals who have learned the power of flight, and that lets viruses that infect us travel the world along with us. As we have unfortunately all learned recently, through several variants.
What this all builds to is not a smoking gun on the origins of SARS-CoV-2, but additional evidence supporting the idea that the features of the virus are found in nature. It is increasingly likely, then, that the virus itself came from nature through human interactions with bats, possibly even without an intermediate animal involved.
While I’ve felt this was the likely origin all along, the evidence coming from rigorous scientific investigation continues to support that narrative, while other origin theories continue to rely on accusations of a massive coverup—because there are no directly supporting facts.
However, since this isn’t a smoking gun on its own, I can’t say we have definitively found the origin of SARS-CoV-2. We’ve just uncovered that the already most likely explanation has even more evidence for its likelihood.

Part of science is identifying and correcting errors. If you find a mistake, please tell me about it.
Though I can’t correct the emailed version after it has been sent, I do update the online post of the newsletter every time a mistake is brought to my attention.
Correction: the caption on a figure in the last issue had a mistake, suggesting that non-ICU patients had the most caspase activation in their T cells relative to healthy controls and ICU patients. This has been corrected in the online edition, now reading: “There are statistically significant differences between all the groups, as noted by the asterisks, with a trend to more caspase activation in patients with more severe disease, as indicated by ICU status”
Thanks are owed to the reader who contacted me about this privately.

What am I doing to cope with the pandemic? This:
Watching: Yellowstone
While I’ve been waiting for episodes of its prequel, 1883, to drop, I’ve been watching the Kevin Costner-headlined TV series Yellowstone. It’s about the Dutton family ranch, Yellowstone Ranch, in Montana (fictional of course), and the tangled, corrupted web that the family weaves to keep their land. I find it compelling, and somewhat reminiscent of a show I thought was a lot of fun—the mystery series Longmire, about a Montana sheriff. Yellowstone is not lighhearted at all, unlike Longmire, but it has a core of interesting characters and has, I think, something to say about a certain kind of American.
On the other hand, it’s another entry in a list of shows I’ve found recently that are, essentially, “Here’s something about a dynastic family full of terrible people doing terrible things to each other.” It’s almost Succession, but with cowboy hats and ranches. Well, more cowboy hats and ranches, at least.
I think it’s worth watching, but it’s not going to cheer you up.

Reader Brock had a question about data accuracy in a world with many kinds of tests:
Do you have any thoughts on how the widespread availability of at-home COVID tests should affect how we look at the test positivity rate? On one hand, if people are using at-home tests and then following up with PCR tests to confirm positives, this would increase the test positivity rate, and what used to be considered a "high" rate might no longer be indicative of a lot of cases that are being missed. On the other hand, the availability of at-home tests might mean that PCR tests are being skipped entirely, and we're just missing lots of cases, so we would be missing lots of cases even when the positivity rate was "low".
I think that this is a meaningful concern. A lot of people are making decisions based on collected public data about infections. On the other hand, hospitalizations are not subject to these data sensitivities, so at least there’s that. To add another other hand, though, hospitalizations are a lagging indicator of outbreaks. There is a solution, though—one that was covered here not too long ago, mentioned in my reply:
Good question. This is yet another reason that I think Dr. Natalie Dean's suggestion of random sampling to assess prevalence is a very good one. There are too many situations where the aggregated data reported from testing entities (including doctor's offices) is too self-selected to be really meaningful. It has a lot of problems--people only testing if they are concerned about COVID, people using home tests, people not being able to even *get* tests.
A random sample approach would resolve most of these problems and give us an excellent prevalence estimate, so I'm increasingly in the camp that local public health authorities should switch to this. Counting positive tests in the aggregate as your chief disease-tracking tool makes sense when you have a few hundred cases worldwide, not a few million.
You might have some questions or comments! Join the conversation, and what you say will impact what I talk about in the next issue. You can also email me if you have a comment that you don’t want to share with the whole group, or if you are unable to comment due to a paywall.
If you liked today’s issue, please consider becoming a paid subscriber and/or sharing this newsletter with everyone you know.
Always,
JS
It’s actually disputed whether he finished or not. Some parts of the attempted canal still exist.

The theories that the virus originated in the wild do not to me explain that the epicenter was in the same city with the leading virology lab. Mere coincidence?
As the son of a philosopher and former biology teacher, I have to harp on a nomenclature and taxonomy matter. (There's a weird sentence!)
Referring to "vaccination" in this context, unqualified, can mislead. Vaccination with US-approved vaccines? AstraZeneca? Sputnik 5? Covovax? CORBEVAX? One of the Chinese vaccines? Cuban? Turkey's homegrown entry?
I speculate from your reference to "one-dose" vaccination not being efficacious, and that the results are from the UK, that it might be US-approved mRNA vaccines plus AstraZeneca, but I don't know. So now I'll check.
[checks]
"Being vaccinated was defined as having two doses of the Pfizer-BioNTech, Oxford-AstraZeneca, or Moderna vaccine or one dose of the Janssen vaccine." So that's a very heterogeneous population, then. The link appears to be a very quick review of 8 studies using the UK's NIH dataset. They don't appear to compare between people who received different vaccines--their result is compatible with, say, AstraZeneca being twice as effective in preventing long-term symptoms as Moderna. (Presumably the underlying studies would have caught that, but it isn't discussed in this particular article that I saw.) There's no mention of people given two different vaccines (booster not matching original shots, say), and obviously they haven't studied any of the newly approved vaccines like Covovax.
Something else I noticed: "The review found that vaccine effectiveness against most post-covid symptoms in adults was highest in people over 60 and lowest in those aged 19 to 35." Interesting. Also weird. Is this perhaps because older folks like me would be more likely to have Long COVID in the first place?