


How do you eradicate polio in New York?
And an update on monkeypox and Rochelle Walensky

Greetings from an undisclosed location in my apartment. Welcome to Viral Transmissions.
Look at me, writing to you two weeks in a row. Thanks to all of you who wrote/liked/commented with well wishes. I am feeling if not 100%, at least consistently above 80% performance reliability.
Today I want to touch on several virus stories that are circulating; first, we’ll discuss the current state of polio spreading in New York State, then the status of monkeypox, and then lastly we’ll touch on the COVID-19 situation, particularly with regard to Dr. Rochelle Walensky, the CDC Director, having come down with mild COVID-19.
This newsletter survives on your enjoyment and the publicity you give it. If you like what I’m doing, subscribe or share—see buttons below to do both.
As a reminder, links that look like this go to the glossary I maintain for this newsletter.
Now, let’s talk viruses.

New York State of Polio
In past issues this summer, I wrote to you about circulating poliovirus and even a case of polio detected in New York State. As a brief reminder, this case of polio was not “wild” virus, but was instead caused by vaccine-derived polio. The oral, live attenuated polio vaccine causes people to shed polio virus. This is not a problem if everyone around a new vaccinee is themselves vaccinated. But this person wasn’t vaccinated against polio—and that oral vaccine hasn’t been used in the US for decades. The patient hadn’t had recent travel, either. We’ll come back to what that means in a moment.
Something else I mentioned at the time was that cases of paralytic polio are a small fraction of overall polio virus infections. Paralysis resulting from polio infection is rare because it requires the virus to jump into the central nervous system, by first leaving the gut, entering the bloodstream, and then traveling along nerves. For this particular gut virus, this process is rare. Most people experience a harmless infection. But, as we’ve seen with COVID-19, if even a small percentage of people experience the worst, that means a lot of people can be harmed.
There are a few things we can learn from all of this information, taken together. A vaccine-derived virus was found in a country that doesn’t use that vaccine—not too surprising considering it is still used in other countries, but a sign that it came here in what was likely a small number of travelers. A symptomatic case of paralytic polio was detected in an unvaccinated person—meaning that there were likely hundreds more infections than just this one case. As New York State health officials have investigated, it has become clear that polio virus is indeed circulating in the state at rates much higher than we would have expected. This is probably, in part, facilitated by the exclusive use of the inactivated polio vaccine in the US, a vaccine which prevents paralytic disease but does not prevent infection. For a country where polio was officially eliminated, this made sense. Unfortunately, with the emergence of this situation, that elimination appears to be in jeopardy.
I’ve written about all of this at greater length before, so now the question is this: so what? What do we do about this in New York, and what do we do if the same situation emerges elsewhere?
Firstly, the state has issued new vaccination guidance, largely focused on people making sure they vaccinate their children, get vaccinated themselves if they aren’t, and complete their vaccination series if it wasn’t completed when they were children: https://www.health.ny.gov/press/releases/2022/2022-09-09_polio_immunization.htm
If everyone follows these instructions, New York could eliminate polio cases, but the circulating vaccine-derived virus wouldn’t go away—because current US vaccines do not prevent the spread of polio, only the disease. Also, that outcome is predicated on a statement that COVID-19 has taught me is a fantasy; “if everyone follows” is not something that happens. Even if antivaccine conspiracy theorists were really rare, a US President once said that “there’s always one [person] who doesn’t get the memo,” and that’s true in public health too.
There is another strategy to consider, though. The oral polio vaccine—the one that led to this virus circulating in the first place—does induce the mucosal immunity that is required to protect against infection. In fact, it’s great at it. If everyone in the US who has been vaccinated with the killed virus had instead been vaccinated with the live attenuated oral vaccine, then this virus would have very few susceptible hosts and would probably burn out.
That vaccine is easy to deploy. It’s not a “jab”; there’s no injection. It’s given in a sugar syrup, not much more complex than simple syrup. Note, though, that I haven’t evaluated whether you can safely add it to a cocktail.
In fact, the CDC is considering using this vaccine again in light of what is happening in New York: https://www.cnbc.com/2022/10/21/cdc-is-discussing-using-oral-polio-vaccine-for-first-time-in-20-years-to-stop-new-york-outbreak.html
The issue here is that using this vaccine lets proverbial toothpaste out of the tube. People who get this vaccine can shed infectious, reverted virus that can cause polio. This virus ends up in the New York State water system. If someone comes from another state who hasn’t had the oral vaccine, they can carry it home with them where it can infect others. If New York State had only a little tourism, I might not think this was a big problem, but it’s a very popular destination to visit.
On the other hand, that vaccine-associated virus is already here in the state. So tourists can come here and get it anyway. Meanwhile, there is a real threat to the state’s residents here and this would improve protection.
In the end I think that the oral polio vaccine will need to be made widely available in the US again eventually, as long as there are holdout antivaccine populations that refuse to protect themselves from this virus. They will continue to act as vectors for this virus, and since the inactivated vaccine doesn’t stop spread, eventually that means someone whose immunity has waned or become compromised is going to get polio. The use of that oral polio vaccine will be a danger to the unvaccinated populations, but they make a choice every day not to be protected—and that choice puts many others in danger. Offering the oral polio vaccine means protecting the rest of us from the consequences of the antivaccine community’s choices.
It’s hard to say how we could ever eradicate polio under these circumstances. Bu at least we can stop its spread and protect vulnerable communities.
Monkeypox update
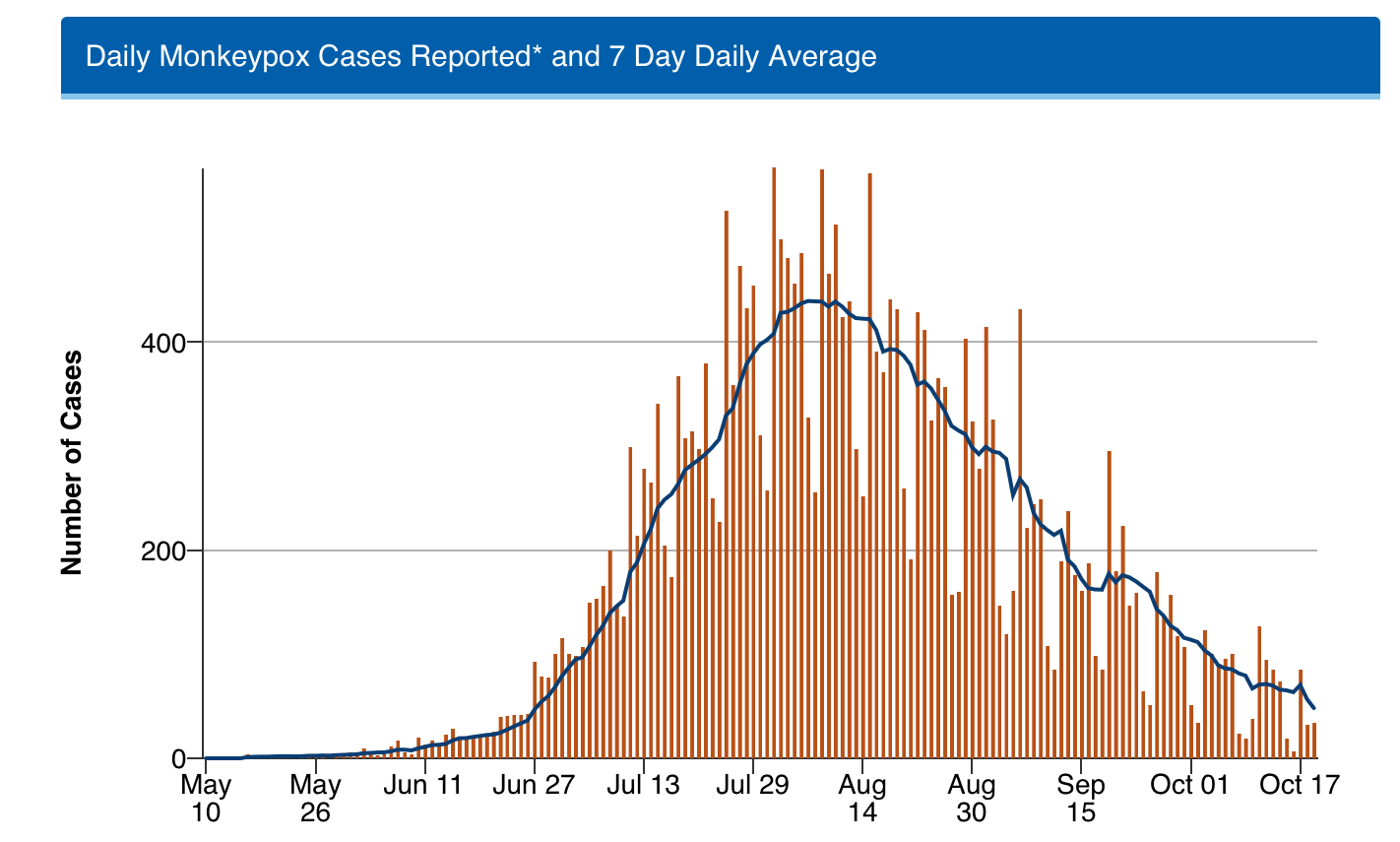
In the time since I last wrote about monkeypox, new cases in the US and around the world have substantially declined. Look at this graph from the US CDC:
The same situation assessment—of a contracting epidemic—has been issued by the European CDC as well: https://www.ecdc.europa.eu/en/news-events/monkeypox-situation-update
Even if we are not testing adequately for this virus—and really, what virus do we test adequately for?—a drop in these numbers this dramatic means the outbreak is starting to recede.
Now, look, this is unequivocally good news, but I want to be clear that these numbers have not reached zero and this virus will continue to be a threat. It is in human communities spreading readily, as people have long feared it could do. So while it is now possibly a less clear threat to the typical person, it is still a present danger.
One thing I do like is the following statement from the US CDC, which makes it clear that this is not just a problem for men who have sex with men:
At this time, data suggest that gay, bisexual, and other men who have sex with men make up the majority of cases in the current monkeypox outbreak. However, anyone, regardless of sexual orientation or gender identity, who has been in close, personal contact with someone who has monkeypox is at risk. Take steps to prevent getting monkeypox. If you have any symptoms of monkeypox, talk to a healthcare provider.
Skin-to-skin contact is what matters for transmission of this. Thankfully it doesn’t do such a great job transmitting and leads to good immunity in most people after recovery. We also have good vaccines against it, albeit in shorter supply than anyone would like. Still, the more that the case spread contracts the more useful that short supply will be.
Anyway, the reality is I don’t think you should have skin to skin contact with people who have obvious pustules on their skin. Also, if you have obvious pustules on your skin, it’s a good idea to see a doctor. This isn’t just monkeypox advice, by the way.
Unfortunately because it can be confused with low-level acne and other skin infections, this isn’t a perfect approach. But definitely we have this one on the run for the moment, if not explicitly getting under control. Long may the trend continue.
Dr. Walensky gets COVID-19 a month after her bivalent booster
COVID-19 is still a threat in the US and around the world. In the US in particular, hundreds of people continue to die every week from the disease and there are new variants out there that can evade preexisting immunity from past infection and cause disease. That preexisting immunity may still offer some protection, but it doesn’t seem to be quite as good without additional repeated exposures to virus antigens through intentional vaccination.
Meanwhile the CDC and the FDA have been encouraging people to get bivalent boosters against COVID-19. I’ve said before that I haven’t seen evidence that these new boosters can stop spread of the disease, but I did say I was hopeful.
Now, there are headlines about the CDC Director, Dr. Rochelle Walensky, getting COVID-19 just a month after she got vaccinated using the new bivalent booster. Of course this has led to some major headlines, and a lot of people questioning what this means for the bivalent booster. So I’ll tell you what it means:
Nothing.
We cannot make conclusions from a single story, no matter how famous the affected person nor how ironic their illness happens to be. Vaccine skeptics will of course exploit these features of Dr. Walensky’s story, but even if the new vaccine prevents 99% of infections, that means 1 in 100 people would be able to get infected after being vaccinated. Dr. Walensky may just have been unlucky.
I think it’s important for the bivalent boosters to be out there, particularly for people who are just now getting their first boosters. I’ve noted before that they are at least as good as the original variety of boosters, and I would bet they are a bit better matched to currently-circulating viruses. I don’t take away any change to that assessment from this story because an anecdote isn’t anything close to data.
Meanwhile the CDC is talking about adding the COVID-19 vaccination to the list of routine recommended vaccinations. This was recommended unanimously by their advisory panel: https://www.nbcnews.com/health/health-news/kids-covid-vaccine-cdc-group-says-add-vaccine-routine-immunization-sch-rcna53129
The misinformation machine, including even major media outlets owned by News Corp, have seized upon a myth here that this means the CDC is now requiring COVID-19 vaccination for children. That is, in fact, a lie.
The CDC does not require any vaccination for anyone, because it doesn’t have the power to do that. Vaccination mandates for children in the US are generally state law, implemented based on eligibility for public school. Unvaccinated children’s aren’t put in jail, they just have to be home schooled for their own safety and that of the children in school. But again, that’s a matter of state law, not CDC recommendations.
All that CDC recommendations mean is this: an abundance of evidence suggests the clear benefit of taking the recommended vaccine compared to the risks of getting g the disease, such that the willful ignorance it takes to avoid the vaccine runs counter to good medical advice. In the case of COVID-19 vaccination, as well as all the other vaccines on the list, that is very much the case.
So, you can certainly decide not to listen to this recommendation, but that choice marks a person who is substantially divorced from reality.
 and a purple heart with an EKG graph on it. Next to the graphic there is the word \"Community,\" which is underlined in red.")
Yesterday was my daughter’s 1st birthday party—she turned 1 quite a few weeks earlier, but the original party date was rained out. Thankfully, she didn’t seem to be aware she turned 1 and was just as happy to (mostly) smear the cake we gave her all over her hands and face yesterday as I imagine she would have been weeks ago.
Regarding my own health and personal situation, thank you everyone who reached out! I continue to feel better and am getting back into the swing of things. Next issue, I think I’ll talk about Ebola viruses. Any other requests?
I want to hear from you, too, with your questions about monkeypox, or COVID-19, or just updates about your lives. This newsletter is a community. Reach out!

I have a commitment to accuracy, but I’m still human and I get things wrong. Sometimes, very wrong. If you catch an error, let me know—you can email me directly or leave a comment.
Thanks for reading today. It’s great to be writing to you again. Have a wonderful weekend!
Always,
JS
In the newsletter you mentioned that next issue, you’ll talk about Ebola viruses.
Currently, there are (as far as we know) five Ebola viruses. For only one Ebola-virus, the Zaire Ebolavirus, there is currently a vaccine available.
Although, there does seem to be a vaccine that targets Sudan ebolavirus from Mercks, that was developed but not tested because there were no Sudan-Ebola outbreaks, see this Science article.
"Merck locates frozen batch of undisclosed Ebola vaccine, will donate for testing in Uganda’s outbreak"
https://www.science.org/content/article/uganda-may-use-destroyed-ebola-vaccine-merck-fight-its-growing-outbreak
Are these five Ebola-viruses so different from each other, and what makes them so different, that the Zaire Ebola-vaccin can´t be used against the other Ebola-strains? I read somewhere that they tested in a lab the Zaire-vaccin antibodies against Sudan Ebola-strain, and they did not react.
One of my comments about walensky was that vax is a dice roll modifier not a force field, so very frequent exposure also matters, and she tended to either not mask or maybe cloth mask in indoor spaces with others.
The timing of her announcement was of course poetic. There was still a whole lot of traffic on Twitter from the day before when she made a post about avoiding c19 that included washing your hands and did not include anything about the air. Not ventilation not filtration not masks.